As we mark a significant milestone – the 5th anniversary of the SASSI Network Blog – we want to take a moment to reflect on the journey we’ve shared with our readers and celebrate the knowledge, stories, and progress made in the field of substance abuse.
Since the launch of the SASSI Network Blog, our mission has been clear: to provide valuable resources that help professionals in the field of substance use treatment, prevention, and recovery. Whether through evidence-based research, real-world case studies, or expert advice, we’ve aimed to create content that educates, informs, and inspires.
Highlighting Our Most Popular Blog Topics
As part of our anniversary celebration, we’re looking back at some of our most popular blog topics over the years. These posts sparked conversations, provided critical insights, and offered practical solutions to some of the most pressing challenges faced by professionals working with individuals impacted by substance use.
Some of these blog topics included:
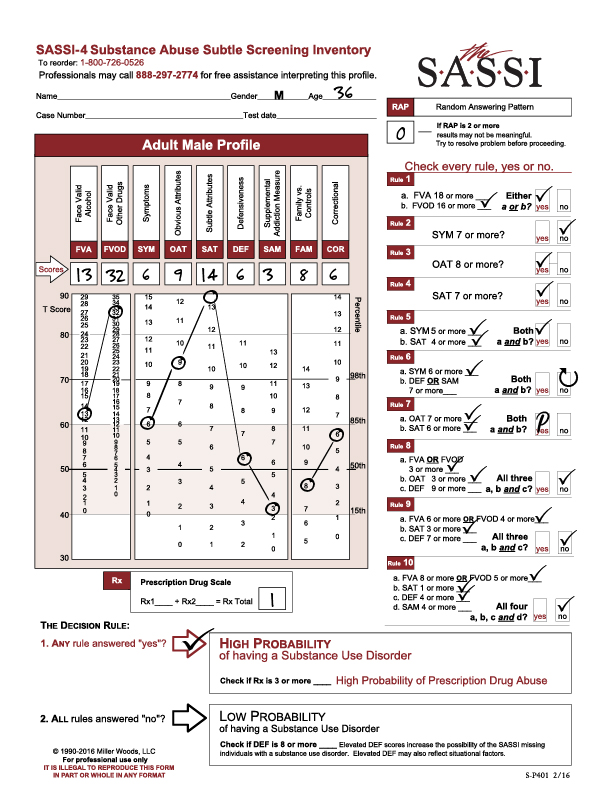
- Understanding the Adult SASSI-4: A deep dive into how the SASSI-4 tool works and how clinicians can interpret results to make informed decisions for their clients.
- The Role of Family Dynamics in Substance Use Recovery: Exploring the often-overlooked role that family relationships play in both the development and recovery from substance use disorders.
- Emerging Trends in Substance Use: Examinations of the latest substances and patterns of misuse affecting communities and how professionals can stay ahead of new challenges.
The Impact of Our Readers
What makes our blog truly special is our community of readers. Over the years, we’ve had the privilege of connecting with professionals who are passionate about making a difference in the lives of individuals affected by substance use disorders. We’ve heard your stories, answered your questions, and learned from your experiences.
Your feedback and engagement have been instrumental in shaping the direction of our content. We’ve been honored to share your successes and challenges as we all work toward creating healthier communities. Your dedication to learning and growth in this field continues to inspire us every day.
Looking Ahead: The Next Chapter
As we look ahead to the next five years and beyond, we hope that the SASSI Network Blog will continue to be a source of knowledge and support. We’re committed to providing content that helps professionals navigate the ever-changing landscape of substance use treatment.
We look forward to continuing our journey with you and exploring new topics, offering fresh perspectives, and delving deeper into the issues that matter most to you.
On this special anniversary, we want to thank you, our readers, for your continued support and for being part of the SASSI Network blog community. Your dedication to improving the lives of those affected by substance use disorders is the heart of everything we do.
Here’s to the next chapter in our shared journey. Thank you for being with us!
Stay tuned for more insightful posts, resources, and updates as we continue to support professionals in the field of substance use assessment and treatment.