We invite you to join us for a free one-hour SASSI Clinical Q&A webinar hosted by our Clinical Director, David Helton, LMSW, LCDC. The Q&A is for anyone new to using the SASSI, those considering using the SASSI, or seasoned veterans at screening with the SASSI. The Q&A is scheduled from 11 am – Noon ET on: July 14th, 2026. You can save your spot by clicking here.
We welcome you to share profiles to discuss with the group by sending them (de-identified) via email any time prior to the session to scarlett@sassi.com. These profiles will help others learn about SASSI and offer insight into the various profile configurations.
Note: Q&A sessions do not provide CEUs and are not a substitute for SASSI Training. To register for a SASSI Training webinar. please visit https://sassi.com/sassi-training-online/.
While the core goal of identifying substance use disorders remains the same, the SASSI-4 (Adult) and SASSI-A3 (Adolescent) are tailored to the very different life stages and behavioral patterns of their respective groups.
Think of it this way: the way an adult hides a drinking problem is often very different from how a teenager masks drug use.
Comparison of SASSI-4 vs. SASSI-A3
Feature
SASSI-4 (Adult)
SASSI-A3 (Adolescent)
Age Range
18 years and older.
13 to 18 years.
Focus Area
Emphasizes long-term behavioral patterns.
Emphasizes family dynamics, peer pressure, and school behavior.
Subtle Items
Focuses on adult stressors like workplace issues and long-term social consequences.
Focuses on “acting out,” rebelliousness, and emotional regulation.
Key Differences in Approach
The Adolescent Version (SASSI-A3)
Teenagers are often in a state of natural rebellion or may be experimenting due to peer influence rather than chronic dependency. The A3 is specifically designed to:
Filter Peer Influence: It helps distinguish between a teen who is “experimenting” because of friends and one who has a burgeoning clinical dependency.
Assess Family Environment: It includes scales that look at the teens’ perception of their home life, which is a major factor in adolescent recovery.
Evaluate “Global” Functioning: It looks at how substance use is impacting their development (school performance, legal trouble, and social skills).
The Adult Version (SASSI-4)
Adults typically have more established defense mechanisms and more to lose (jobs, marriages, custody). The SASSI-4 was recently updated to better capture:
Prescription Medication Abuse: Since the opioid crisis, the adult version has been refined to better identify those misusing legal prescription medications.
Severity Markers: It provides more nuance on the intensity of the disorder, which helps in planning for long-term recovery versus short-term intervention.
Why the Distinction Matters
Using an adult test on a teenager (or vice versa) could possibly lead to inaccurate results. A teenager’s natural impulsivity might look like a “disorder” on an adult scale, while an adult’s more calculated “denial” might not be caught by a test designed for a more impulsive adolescent.
The purpose of the SASSI is to help identify people who are likely to have substance use disorders so that early intervention and treatment can be initiated when appropriate.
The Substance Abuse Subtle Screening Inventory (SASSI) is a widely used psychological screening tool designed to identify individuals with a high probability of having a Substance Use Disorder (SUD).
Its primary value lies in its ability to look past “denial.” Many people struggling with addiction may not be ready to admit it, or they might intentionally try to minimize their usage during an evaluation. The SASSI helps by being a bit more “clever” than a strictly face-valid questionnaire.
How It Specifically Helps
1. Identifying “Hidden” Issues
Unlike many tests that ask straightforward questions (e.g., “How many drinks do you have a week?”), the SASSI includes subtle items. These are questions that don’t seem related to substance use but are statistically linked to the behavioral patterns of people with SUDs. This helps clinicians identify people who are:
In deep denial.
Intentionally hiding their use.
Unaware that their behavior constitutes a disorder.
2. Providing a Faster Path to Treatment
Because the SASSI is relatively quick to administer and score, it acts as a “triage” tool. It allows counselors to quickly decide who needs an intensive clinical interview and who might just need basic education. This efficiency ensures that resources go to the people who need them most urgently.
3. Objective Data for Referrals
Objective scoring of the SASSI yields a screening outcome – a yes-or-no answer as to whether the client has a high probability of having a substance use disorder, as well as a check on validity of the profile, a score indicating level of defensive responding, and a score indicating the possibility of prescription drug abuse. For people involved in the legal system (like DUI cases) or workplace evaluations, having objective, validated results remove personal bias from the evaluator. It provides a foundation for recommending specific levels of care, such as:
Outpatient counseling.
Intensive Outpatient Programs (IOP).
Inpatient detoxification.
What the SASSI Is Not
It is important to remember that a high probability of a substance use disorder result on the SASSI is not a final diagnosis. A licensed professional must still conduct a full clinical interview to make an official diagnosis based on the DSM-5-TR.
Overall, the SASSI provides a useful tool for healthcare providers, substance abuse professionals, criminal justice entities and others who are involved in identifying and treating substance use disorders. It can help to ensure that individuals receive appropriate care and support, which can ultimately improve their health and well-being.
Many people know that the SASSI is possibly the best substance use disorder screening tool that exists in the behavioral health field today. The instrument can be easily administered in 15 minutes or less and manually scored in less than two minutes (or scored automatically in the online web-based version), resulting in an objective empirically-based statement of the likelihood of the client having a substance use disorder with an overall accuracy of 92% for adults and 89% for adolescents. And it achieves this kind of accuracy even in clients who are unwilling or unable to acknowledge their substance misuse or the symptoms associated with it!
Through extensive case study research, the SASSI has been found to be able to provide even more utility to clinicians in the form of clinical interpretations that go beyond just the high or low probability of a substance use disorder result. In addition to interpretations of individual scale raw scores that fall outside the boundaries of the research-based established normal distribution, we also have discovered some trends or characteristics in the specific situation in which the client scores as high probability of a substance use disorder based on SASSI decision rules that involve only subtle scales rather than face valid scales. That is the subject of our blog today.
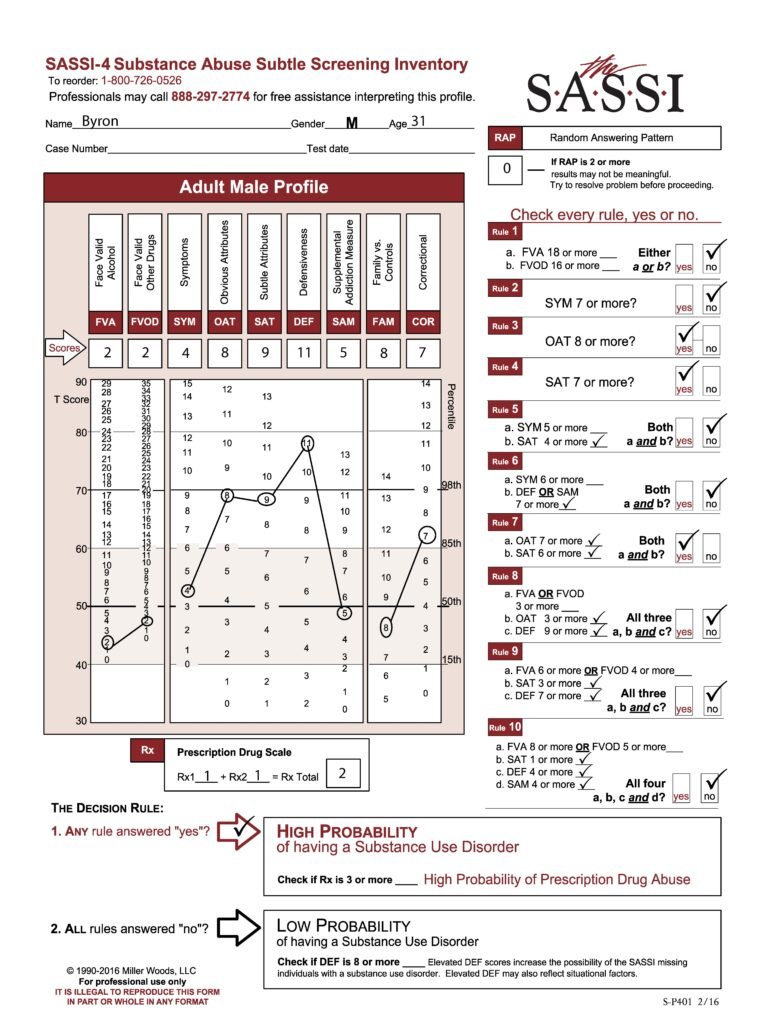
The SASSI is made up of both face-valid scales and subtle scales. Face-valid scales such as FVA, FVOD and SYM are scales that are very obvious about what they are measuring, while subtle scales such as OAT, SAT and DEF are made up of items that do not seem to have anything at all to do with substance use. Our case study analysis showed that certain behaviors, characteristics or patterns emerge in individuals who score as high probability based only on subtle scales. Let’s take a look at an example. Byron is a 31-year-old male who was asked to be evaluated because of a child custody battle in which the mother alleges that Byron misuses drugs. Byron has not yet had a comprehensive assessment done, but has so far only admitted to some occasional use of marijuana. A SASSI was administered and the results showed that Byron met the criteria for Decision Rules 3, 4 and 7. Each of these decision rules involve only subtle scales and no face-valid scales. So, what characteristics do we tend to find in individuals with this type of scoring pattern?
One key feature of this type of scoring pattern is the fact that these individuals often have very little insight into the pervasive nature of the addictive disorder in their lives. Most of the time, this type of client actually has a very sincere delusion regarding their substance misuse. In other words, they are not trying to trick you into thinking they do not have a problem with substances; they simply do not see it. Often, every single activity this person is engaged in and every decision they make somehow involves substance use. Often, the substance misuse has become an unhealthy way to cope with emotions that are too overwhelming and so individuals with this type of scoring pattern are very emotionally avoidant. Many times, this individual has difficulty admitting their weaknesses or the personal limitations with which they struggle and instead choose to focus on very superficial things, ignoring the depth of the substance problem in their life. We can see these types of traits and behavior patterns manifested in this client’s individual face-valid scale scores such as lower than average (T-score of 50 is the mean) FVA and FVOD scores and only an average SYM score. These all indicate a client who does not acknowledge or admit to having any significant problems or negative consequences as a result of substance use. The client’s extremely high DEF score indicates a very high level of guardedness and the desire to be seen as having no weaknesses or faults. It’s even possible that the FVA, FVOD and/or SYM scale scores could be artificially low because of minimization of symptoms in the client’s answering patterns on these scales fueled by this defensiveness. However, as mentioned previously, it’s possible and even probable that this client really has very little insight into his problem with substance misuse and so he may be unable to even recognize the obvious negative consequences he is experiencing. This is especially typical of clients with high SAT scale scores as this client has. While this client does also have an equally high OAT score, which often indicates some ability to recognize negative attributes that are common in individuals with substance problems such as impulsiveness, self-pity, resentment, and impatience, it is more likely in this case that the client does not see these issues as having any relationship to his misuse of substances.
At this point, a comprehensive assessment needs to be done along with a formal diagnosis and possible treatment plan formulated. Since the SASSI does not provide an actual diagnosis and does not, by itself, indicate a need for treatment or the level of treatment, it is important to gather more information such as self-reports of the client’s current usage patterns, collateral reports, naturally occurring records, behavioral records, etc. to determine a diagnosis and course of action. Typically, clients with this scoring pattern do have a significant substance use disorder and many of them, if they need treatment, will often need a relatively intensive level of treatment which includes individual and group therapy sessions; more than just cognitive/educational programming. However, individuals with this type of scoring pattern will often be initially resistant to any treatment as they honestly do not see a problem that needs to be treated. The high level of defensiveness will require lots of time spent in developing a therapeutic alliance and positive rapport, affirming and supporting him throughout the process. Clients like this are often a high relapse risk and so it is important to provide wraparound supports and a level of intensity in the treatment regimen which allows for quicker and stronger intervention in the event the client attempts to relapse. Individuals who score as high probability of a SUD based only on subtle scales are often some of the most challenging clients, but with information gained from the client’s scoring patterns on the SASSI combined with additional information from other sources, you are in a better position to know what to address to increase the possibility of success with this client.
Don’t forget that full training on administering/scoring the SASSI and clinical interpretation of the sub-scales is available. Check out https://sassi.com/sassi-training/ to register for an upcoming training. Also, our free Clinical Helpline is available M-F from 1:00pm to 5:00pm EST to answer any questions you have about the SASSI.
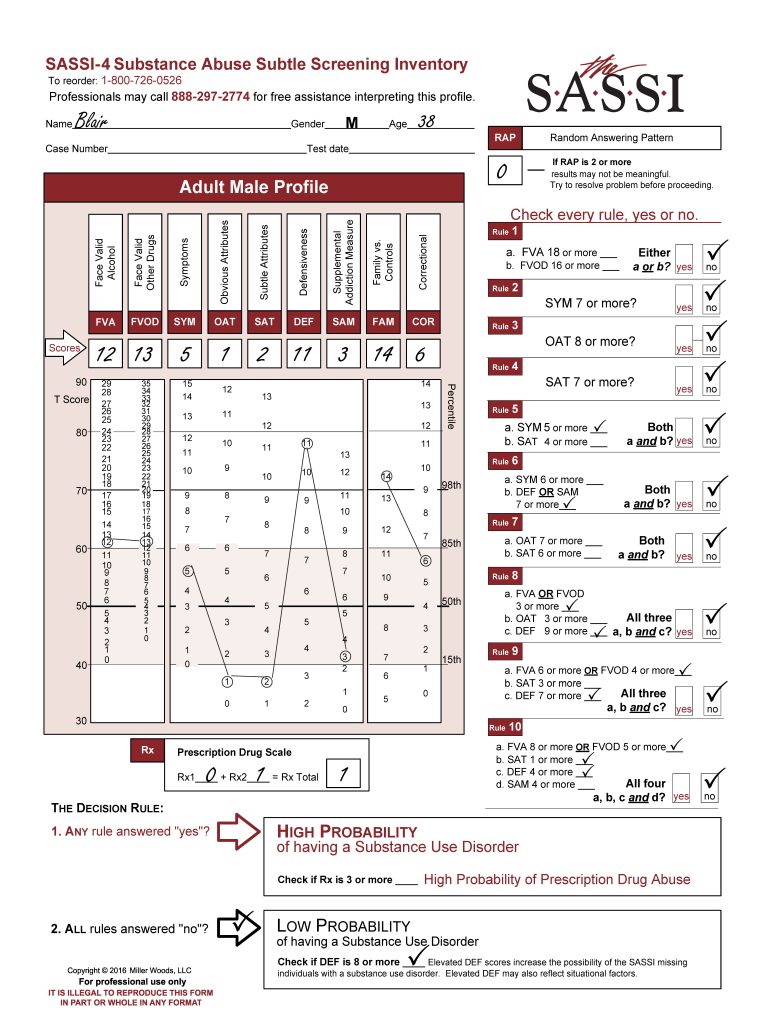
The following profile is for a 38-year-old male, “Blair,” who has been mandated to counseling following an instance of spousal abuse. First, note that the scale scores do not meet the criteria for classifying Blair as High Probability of having a substance use disorder (SUD). However, the Face-Valid Alcohol (FVA-12) and Face-Valid Other Drugs (FVOD-13) scores are moderately elevated above the mean (50th percentile) since they are more than one standard deviation from the mean and above the 85th percentile. It is important to recognize that FVA and FVOD are not just measures of frequency and quantity of consumption. Rather, they are mostly measures indicating acknowledgement of significant negative consequences as a result of substance misuse, as well as possible loss of control and using as a coping mechanism. Thus, even moderately elevated scores that do not in and of themselves lead to classifying the person as high probability of having a SUD are often indicative of some level of substance misuse. It is important to investigate this further. We not only want to establish whether substance misuse is a current or past pattern of use, but (in the context of this client’s reason for referral) further investigation is also needed to determine more about the relationship between physical abuse and substance misuse in this client’s life.
Note that the Obvious Attributes (OAT-1) score is low, i.e. it is below T40 where less than 15% of the normative sample typically scores. This type of OAT score suggests that Blair does not acknowledge the typical negative attributes or behaviors commonly associated with substance misusers such as impulse control problems, low frustration tolerance, impatience, a tendency to hold grudges, etc. An OAT score this low suggests it is not simply that he does not perceive himself as engaging in such behaviors, but that he actively (consciously or unconsciously) distances himself from any hint that he has such tendencies. In other words, he finds it difficult to acknowledge common weaknesses, personal limitations or human foibles and certainly does not see himself as being in any way similar to those who have substance problems. Often, people who come from homes that were dominated by abuse, substance misuse, or other problems are motivated to see themselves as not being like the primary abuser in their family of origin. His very elevated FAM score (FAM-14) and to some extent his somewhat elevated SYM (SYM-5) score suggest that he may have lived in an environment affected by substance misuse.
The Subtle Attributes (SAT-2) score is also significantly below average, and this can often indicate a person who may exhibit strong feelings of hypersensitivity to what others think of him stemming from his perception that others frequently reject him and unfairly judge and criticize him. This score suggests that Blair may be highly attuned to others’ opinions and may perceive slights or criticism, even when none are intended.
The Defensiveness score (DEF-11) is very significantly elevated. This often indicates someone who has their guard up and answers the questions by endorsing only things that may make them look more positive. This is not particularly abnormal in cases like Blair’s where there are situational factors putting him at risk of losing something important to him. Since Blair is being evaluated following an accusation that he beat his spouse, he is naturally on guard. The defensiveness could also reflect a more general tendency to avoid seeing and acknowledging any personal limitations or weaknesses and is somewhat confirmed by his very low OAT score as discussed earlier. Regardless of the cause, it is important to recognize that Blair probably approached the screening process in a defensive manner and because of this there is also a higher-than-normal possibility of a false negative and potentially a possibility that Blair minimized some of his symptoms of misuse on the more face valid scales such as the FVA, FVOD and SYM.
As mentioned earlier, Blair’s score on the Family vs. Controls (FAM-14) scale is significantly elevated. The FAM scale is composed of items that tend to identify individuals who may have been involved in a family of origin in which there was significant substance misuse. People who have high FAM scores often may obsessively focus on the needs and feelings of others. It is therefore interesting to contemplate how a high FAM score might fit as a characteristic of a perpetrator of domestic violence since spousal abusers are not generally thought of as “caretakers.” The crucial element may be the tendency of individuals who score high on the FAM scale to base their happiness and their sense of well-being on the behavior of others, leading to a need to control. Violence can be an extreme expression of a profound need to control.
Based on his SASSI scores, the Decision Rules result indicates a low probability of Blair being diagnosed as having a SUD. However, the significantly elevated DEF score cautions that there is an increased possibility of a false negative result (i.e. test-miss). His FVA and FVOD scores, while not high enough by themselves to provide a “high probability of a SUD” result, were clear indicators of acknowledged negative consequences from misuse of substances. Given the fact that many people with DEF scores as high as Blair’s often minimize some or a lot on the face valid scales to make themselves look better, there is still a possibility that Blair may suffer from a substance use disorder. Substance misuse is a common ingredient in domestic violence.
Domestic abusers often do not assume responsibility for their behavior, claiming that the victim “made me do it.” Blair’s SASSI profile corroborates and expands on this. The low SAT score suggests that Blair may have this victim mentality, and the low OAT score suggests that he is indisposed to see in himself the very tendencies that are likely to lead to spousal abuse such as low frustration tolerance, poor impulse control, anger management problems, a tendency to hold grudges, etc. The high-DEF score suggests a broader proclivity not to acknowledge personal limitations and to only endorse positives; and an extreme focus on others, as suggested by the high FAM score, could lead to an inability to deal effectively with interpersonal conflict. Ongoing comprehensive assessment should be directed toward determining more precisely the role of substance misuse in Blair’s spousal abuse. Treatment should also be directed toward helping Blair perceive and act in accord with appropriate personal boundaries. He is likely to need help in learning to accept and deal with interpersonal conflict and to assume greater responsibility for his behavior. As it stands, his extreme need to control others may lead to poor social judgment that allows him to construe violent acts as mature behavior and provides him with a rationale for excusing the inexcusable.
We hope you find this useful information regarding clinical issues. As always, the Clinical Helpline at 888-297-2774 is open to serve you Monday through Friday, 1 pm to 5 pm (EST).
Identifies high or low probability of substance use disorders in adults 18 and older and includes a prescription drug scale that identifies individuals likely to be abusing prescription medications. It also provides a measure of profile validity and clinical insight into level of defensiveness and willingness to acknowledge experienced consequences of substance use disorder.
Identifies high or low probability of substance use disorders in adolescent clients ages 13-18. It also provides clinical insight into family and social risk factors, level of defensive responding, consequences of substance misuse teens endorsed, and a prescription drug abuse scale that identifies teens likely to be abusing prescription medication.
A Spanish language screening instrument empirically validated in clinical settings for use with Spanish-speaking adults from diverse ethnic backgrounds.
Identifies preintervention risk of future impaired driving, and changes in DUI-related risky behaviors & attitudes following intervention. Ideal for initial risk assessment, pre and posttest screening, and program evaluation.
We invite you to reach out to us for additional information and with any questions you may have at 800.726.0526. Training is available on all instruments.
In our last blog we discussed a profile with defensive responding on the SASSI. In this blog, we would like to discuss strategies for handling clients who respond in this manner and the steps that might be taken to reduce defensiveness prior to administration of the SASSI.
The two factors most frequently related to defensive responding are 1) the purpose of the evaluation – i.e. to determine if there is a high probability of a substance use disorder and 2) the context or setting in which the evaluation is taking place – i.e. situational factors that may result in serious consequences for the individual such as jail time, loss of a job or loss of child custody. While there may be little that can be done to change the reason for a SASSI screening, there are a few things you can do to reduce the effect of the stigma and fear that many individuals feel in legal, EAP, or child welfare settings. Research suggests that professionals working with a client in any setting are more likely to have positive successful results with that person if they are able to develop a positive rapport with them. Specifically, you can help the client view your role as one of a helping professional who values them as an individual, recognizes and is empathetic to the difficulty they are currently facing and desires not to punish or demean them, but to assist in getting them any help they may need.
Building rapport with a client before presenting the SASSI to them can be as simple as meeting them in the lobby, smiling at them genuinely, asking about their well-being, and spending some time talking to them in a manner that you would use with anyone you were interested in getting to know better, rather than immediately “getting to the business” of the trouble that brought them there. Talking to the client in this friendly, engaging and empathetic way can be useful in helping the client to develop a higher level of trust in you, to lower their defensiveness, and to be more forthright and honest in their answers on the SASSI questionnaire. Using this procedure gives you a chance to put the client at ease and reduce any perceived threat by beginning to develop a trusting and empathic relationship. Letting clients know that you understand their pain and acknowledging how scary it must be to go through this process will also help to reduce the fear and apprehension that often leads to defensive responding.
Additionally, clinical experience has shown that clients tend to respond less defensively when told in advance that they will have a chance to talk over their answers to the questionnaire with you after they’ve finished. Letting the client know upfront that you will discuss their responses with them after they finish gives clients the message that you view them as important and value their input and perspective. One very common fear among mandated clients is that they will be mistakenly or unfairly judged by a system that doesn’t care much about their well-being. If clients know that you are someone who will not jump to conclusions and are willing to listen to their point of view, they will usually have less of a reason to feel threatened. Letting them know that the questionnaire is simply a way for you to get to know them better and to find out what problems, if any, you can help them with, as well as telling them that there are no right or wrong answers increases the likelihood that they will respond in a more open and forthright manner. It is also often useful to refer to the SASSI in terms that are not perceived as negative such as “questionnaire” rather than “test”; “survey” rather than “screening instrument.” Taking these steps will help to ensure that clients will be more open to hearing your feedback and comments when it is time to review the SASSI results.
In short, the two most effective ways to reduce the likelihood of defensive responding on the SASSI are to 1) spend some time building a positive trusting rapport with the client before ever introducing the SASSI or talking about why the client is seeing you, and 2) administer the SASSI in the context of an empathic and trusting relationship and let the clients know that they will have a chance to review the results with you.
If you would like to discuss any of your clients screening results, feel free to call the free clinical helpline at 800-726-0526, option 2.
The profile being discussed is for Julia, a 21-year-old single parent female, who is participating in mandated counseling following an allegation that she has been neglecting her child. The child was removed from her care and placed with family members temporarily. This counseling will play a major role in her being allowed to resume custody of her child.
There is probably no circumstance more likely to evoke feelings of defensiveness in a person than revealing the details of personal, family life, and private attitudes for others to scrutinize, particularly when other people are given the power to determine an individual’s parenting abilities and possibly remove one’s child from custody. It is no surprise then that Julia’s DEF score is elevated, given the difficult situation she is in. In reviewing Julia’s SASSI scores, she does not meet the criteria for classification as High Probability of having a substance use disorder (SUD). While elevated DEF scores, when coupled with a Low Probability result, can potentially imply an increased possibility of the SASSI missing an individual with an SUD (a false negative), an elevated DEF may also reflect serious and difficult situational factors facing Julia with custody of her child at risk.
The most striking and important feature of her profile is that most of her individual scale scores are rather “flat”, not really deviating very far from the mean (T Score of 50), which is where most average people would score. Besides the DEF scale score, only the COR score is significantly elevated. This suggests that overall she responded in a generally “average” way (answering similarly to people not in treatment for SUD). The two exceptions are DEF and COR.
Her high DEF score indicates a possible tendency to endorse only things that make her look good to others, to have her guard up so as to not reveal anything about herself that may be viewed as negative. Again, when one is being accused of child neglect and one’s child could be removed from the parent, it is quite normal for that parent to have their defenses, their guard way up and not want to show any weakness or negative traits, even though all humans have weaknesses with which they struggle. Therefore, this high level of defensiveness could be seen as entirely situational or perhaps even a personality trait. In addition, it is noted that while Julia’s DEF scale score is very high, her SAM scale score is not at all high. Prior case studies reveal to us that often when a person has a high DEF scale score and also has a high SAM score, this could be an indicator that the person’s defensiveness may be related to substance abuse. That is not the case here though. It is therefore most likely that her defensiveness is more general and situational rather than being specifically related to substance misuse.
Julia also had a very high score on the COR scale. While this score has nothing to do with the SASSI decision rules leading to a result of high or low probability of a substance use disorder, our experience with high COR scores indicates that a person with high COR scores is answering the questions on that scale very similarly to the way a person with a long history of criminal justice involvement would answer. Therefore, a person with a high COR scale score could be at greater risk of engaging in behavior that may get them arrested. Sometimes certain personality traits of the individual can be found in clients with high COR scores that may contribute to their risk of acting out and being arrested. Therefore, it is often recommended that the therapist explore for signs of low frustration tolerance, anger management problems, poor social skills, poor impulse control or being one who enjoys engaging in high risk behaviors and add these to the treatment plan to try to lower risk.
In summary: While Julia is alleged to have engaged in child neglect, there can be many reasons why a parent may engage in this behavior, with substance abuse being only one of them. As the SASSI is not designed to be a measure of a wide variety of pathologies, but is limited to the role of determining the likelihood of a substance use disorder, the results indicate that substance use disorder is not likely.
It is important to acknowledge the reality of the fear and pain underlying defensive responding on the SASSI. In order to do so, it is valuable to have a good understanding of the nature of your client’s defensiveness. There is no clear evidence in this case that defensiveness is an ongoing characterological feature or personality characteristic of Julia. Her defensiveness therefore is likely to stem from situational factors. Having said that, her high COR score indicates potential risk of engaging in behaviors that could cause her to get in trouble which may be fueled by difficulty controlling her anger and frustration and may cause her therefore to display poor judgement and act impulsively. These potential issues could indeed put her child at risk as well as herself and so should be explored carefully.
Be sure to read our next blog which will discuss tips for reducing defensiveness.
As always, feel free to call our free clinical helpline M-F 1-5 pm ET for assistance in administering, scoring, and/or interpretation of profile results at 800-726-0526 Option 1.
We want clinicians to find the SASSI to be helpful in their work in a way that enables them to affect the lives of their clients in a positive manner.
When a client is unable to acknowledge (sincerely deluded) or unwilling to accept they may have a problem, a clinician’s skillful and caring feedback on SASSI results may help break through those barriers and enable the client to take the courageous step toward recovery.
If you would like to learn more about clinically interpreting SASSI profiles, we encourage you to join us for one of Clinical Interpretation trainings. For more information on live, on-demand, and in-person workshops, please visit https://sassi.com/sassi-training/
Free assistance interpreting SASSI results is available M-F 1-5 pm ET at 800.726-0526 Option 2.
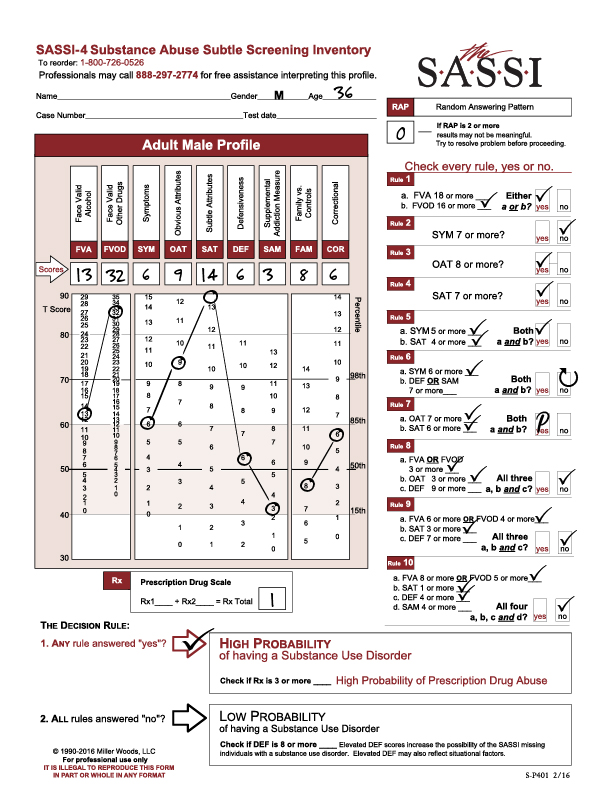
The following profile result is of a 35-year-old male referred for screening and possible assessment after a drug-related arrest. He completed the FVA/FVOD side of the questionnaire based on his entire life timeframe. His RAP score was 0, indicating no random responding and that the result should be valid. His Prescription Drug Scale score (Rx) was 1, so he did not meet the cutoff for High Probability of Prescription Drug Abuse.
Looking at this profile, we see that he was classified as high probability of a substance use disorder based on the following Decision Rules:
Decision Rule 1 with a FVOD score of 32.
Decision Rule 3 with an OAT score of 9.
Decision Rule 4 with a SAT score of 14.
Decision Rule 5 with a SYM score of 6 (5 or more) and a SAT score of 14 (4 or more).
Decision Rule 7 with an OAT score of 9 (7 or more) and a SAT score of 14 (6 or more).
Looking at the graph on the SASSI Adult Male Profile sheet, we see an extremely high elevation on the FVOD scale score which is significantly above the 98th percentile. Individuals who score this high on the FVOD are able to acknowledge currently having or having had numerous negative consequences and problems as a result of their use of drugs. This can include loss of control of the drug use as well as using a coping mechanism. It is important to note that, since he was asked to use the “entire life” timeframe for the FVA and FVOD scales, his admission of having these consequences and problems with drugs may be related to some time in his past and not necessarily currently. For example, the client’s score on the SYM scale (which is similar to the FVA/FVOD in what it is measuring), is not nearly as elevated as his score on the FVOD even though the questions are not that dissimilar from the FVOD questions.
This suggests that he is not showing as much acknowledgement on the SYM scale of the symptoms of substance misuse that he admitted to on the FVOD scale. This could be related to the fact that the SYM scale (like all scales on the True/False side of the questionnaire) has no specific timeframe associated with it and therefore the client may have the belief that, while he has had significant problems with drugs in the past, he may not believe his current drug use is as much of a problem currently. It is highly recommended that clinicians do a content analysis of the client’s answers to the FVOD and SYM scale questions as this will provide more insight into the client’s acknowledged problems with drugs.
This client’s elevated OAT scale score, like the elevated FVOD scale score, suggests a capacity to acknowledge and identify with many of the typical negative attributes (general personality and behavioral characteristics) and personal limitations that are often common among those with substance use disorders – e.g. impatience, resentment, self-pity, impulsiveness). While the client can often see these “character defects”, they may not always feel motivated to change them or feel capable of changing. Given that the OAT score in this case is above the 98th percentile, it is highly probable that this individual may be able to closely identify with individuals in recovery from substance use disorder, such as those found at recovery support groups, and therefore may be more willing to trust these recovering individuals and follow their recovery advice.
The client’s highly elevated SAT score (the highest score on this profile), which is higher on the graph than the OAT score, suggests that despite the client’s capacity to acknowledge the more obvious problems and negative consequences associated with his use of drugs, there are subtle aspects of his behavior, personality, and addiction that are extremely hard for him to acknowledge. In other words, he may not be able recognize the pervasiveness of his addiction, how it negatively affects and rules every aspect of his life with deeply held negative thinking patterns, beliefs and negative coping patterns driving his addictive behaviors.
Clients with a pattern of scores like this client who tend to be able to acknowledge heavy usage, negative consequences and problem behaviors, may still be convinced, sincerely deluded into thinking that they are not truly addicted. They will often present as more “superficial” saying things like “well, I go to work every day and do my job so I couldn’t be addicted”. Clients with elevated SAT scores (especially higher on the graph than their OAT score) tend to be more initially resistant to the need for treatment and are more likely to relapse. These clients tend to be detached from their feelings and have relatively little insight into the basis and causes of their problems (namely substance addiction). These clients typically need a more intensive level of treatment where they can receive constant support for their recovery efforts and can get the kind of group processing therapy needed to help them connect with their feelings and learn how to cope with them without drugs.
In providing treatment to this type of client it is important to recognize that underneath the many excuses (other than substance addiction) for their problems, there is an individual with a substance use disorder who is likely in pain and scared. Individuals with high SAT scores may not be in touch with the pain and fear, largely because they immediately numb any negative feelings with substances as soon as they appear, but the pain and fear. In this case, intensive treatment and group work has to be accompanied by sensitive and skillful clinical intervention that lets the individual know that somebody is aware of their fear deep within and that it will be a relief to let it out to begin healing.
We hope you find this useful information regarding clinical issues. As always, the Clinical Helpline at 888-297-2774 is open to serve you Monday through Friday, 9 am to 5 pm (EST).