Perplexed callers periodically raise the question of how to interpret the results to their clients when all the scores fall within the norm and are only one standard deviation above or below the T-score of 50. Clinical interpretation is minimal although you can glean some useful information than just reporting a high probability.
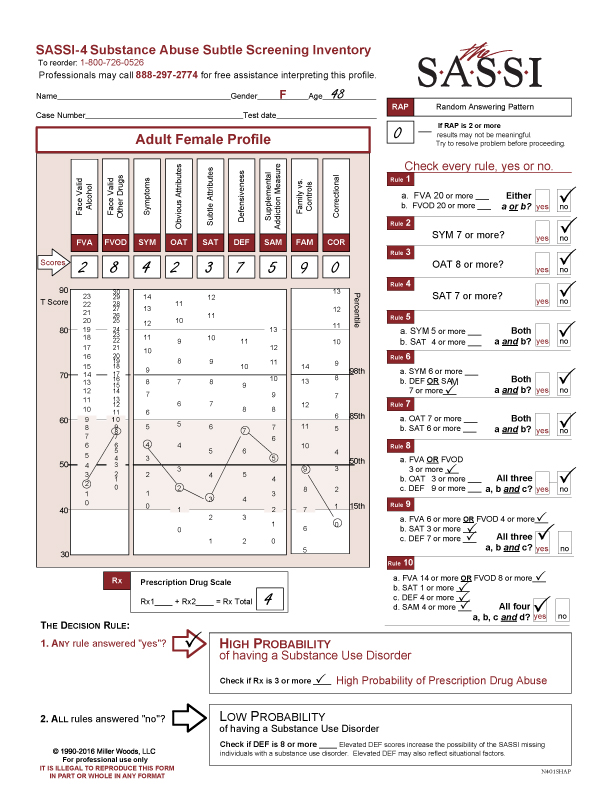
The following profile result is of a 48-year-old female. She completed the FVA/FVOD side of the questionnaire for the last 12 months. Her RAP score was 0. Her Prescription Drug Scale score was 4 which indicates a High Probability of Prescription Drug Abuse.
As you can see, her FVA of 2 indicates below average use of alcohol, her FVOD score of 8 indicates above average use of drugs though within the norm. Her SYM score of 4 is also within the norm and although above average, she is not endorsing a lot of negative symptoms or consequences of her usage. Content analysis is useful with the Face Valid scales because they will give the context or conditions of how the client is using substances. The OAT score of 4 is within the norm so one hypothesis to explore, given the High Probability of a Substance Use disorder result, is if this client identifies with other addicted folks and those issues we often see in that population i.e. self-pity, resentment, low frustration tolerance, impatience etc. I would suspect not.
The SAT score of 3 is well below average although within the norm, this client may be concerned with what you think about her. The DEF scale score of 7 is above average but also within the norm so you may be picking up a bit of a defensive posture with this client.
The last 3 scales, SAM, FAM and COR have no clinical impact.
Moving onto the Rules, two rules are met: Rule 9 and Rule 10.
Rule 9
FVA 6 or more or FVOD is 4 or more
SAT is 3 or more
DEF is 7 or more
All three, a,b, c ? YES
Rule 10
FVA is 14 or more or FVOD is 8 or more
SAT is 1 or more
DEF is 4 or more
SAM is 4 or more
All four, a,b,c, d ? YES
The Rules are research based. Single scores within one standard deviation above or below the normative scores for each scale are not likely to indicate strong evidence of a diagnosable substance use disorder or a clinical problem. However, validation research indicated that some combinations of scores within this normative range such as in Rules 9 and 10 were evidenced by people who were diagnosed with a substance use disorder, and yet this same pattern of scores was not evidenced by those without substance use disorders. The scoring rules identify patterns of scores that accurately and reliably identify individuals with substance use disorders- even when the individual scores in the rule are not indicative of SUD on their own. Also, Table 10 in Chapter 7 in the SASSI-4 User Guide & Manual shows that both Rules 9 and 10 have a 96% accuracy rate indicating that the rules rarely identify people who do NOT have an SUD as positive on these rules.
You can see for Rules 1-4, the cutoff scores are outside the standard deviation which allows for both meeting the rule criteria and allows for easier clinical interpretation as well.
It is also important to note that the cutoff scores for each scale in any rule are specific to the rule. Being close doesn’t count.
Giving feedback to this client, the administrator needs to be aware of the bit of defensiveness and sensitivity of the client and perhaps the reluctance to identify as an addict. Using the information, she did endorse in the FVA, FVOD and SYM scales along with the Prescription Drug Scale results. It may help her to connect the dots and thus become open to whatever treatment considerations are discussed.
As always, if you have any questions about your SASSI results, please contact us through the free Clinical Helpline. We are available M-F, 12 – 5 EST at 888-297-2774 or 800-726-0526.
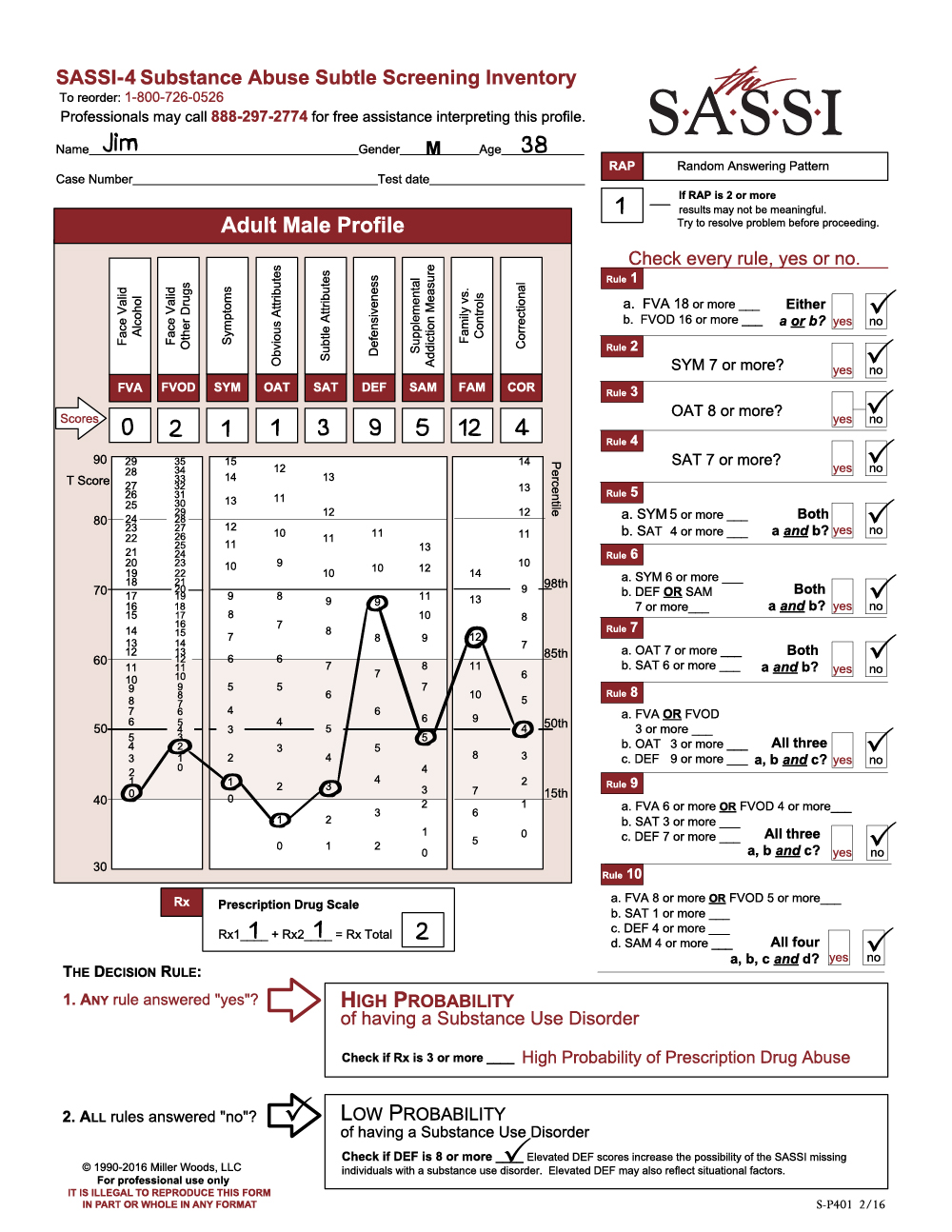
The client is a 38-year-old male named Jim (not his real name), who was referred for a substance use evaluation following a second arrest for domestic violence. The practitioner calling in the profile reported having collateral evidence substantiating a significant history of alcohol abuse for this client.
The SASSI results indicate that Jim has a low probability of having a substance use disorder. He is not acknowledging any significant problematic use of alcohol (FVA=0) or other drugs (FVOD=2). In fact, he denies having any of the symptoms commonly associated with individuals who have substance use disorders (SYM=1). However, note that Jim’s responses are highly defensive (DEF=9) and significantly similar to individuals who are instructed to minimize and conceal problems. Given that his report on the FVA and FVOD is in direct conflict with information from other sources, it is likely that he is minimizing the degree to which he has experienced alcohol and other drug problems or related symptoms. This increases the risk that the SASSI classification of low probability may be in error – in other words, the accuracy of the decision rules may be slightly decreased. As in most assessment situations where the client is relatively defensive, augmenting self-reported alcohol and drug history with data from external sources is advisable before ruling out substance use problems.
Experienced SASSI users working in criminal justice, EAP, DOT, child protection, and other similar settings will recognize this profile as relatively common for clients who are mandated for assessment. Indeed, Jim has been charged with assaulting his partner for a second time. One possibility is that he fears a harsh punishment may be coming if he does not present himself in a favorable way. He may also be convinced that he is not to blame for his behavior, explaining that his partner provoked him or that he was acting in self-defense. While the SASSI does not reveal the exact cause or reason, the high DEF score is a strong indicator that Jim approached the assessment in a defensive manner.
Notice also that Jim’s OAT score is significant given that it falls below the 15th percentile (OAT=1), meaning that only 15% of the general population would score this low. A score in this range usually indicates a person does not identify with any of the problematic behaviors typically associated with substance abuse (for example, anger management problems, negativity, self-centeredness, etc.). Jim is not likely to acknowledge having these behaviors and probably wants to be viewed as being completely different from people who do. Individuals with a family history of addictive or violent behavior often cope by distancing themselves from the addict or perpetrator as if to say, “I’m nothing at all like my alcoholic mother or physically abusive father.” In fact, the caller reported that Jim’s mother is an active alcoholic.
Jim’s FAM score of 12 is also significantly elevated (above the T 60 line or the 85th percentile). His responses are similar to family members of substance dependent individuals. It is likely that he shares many of the characteristics and traits commonly associated with individuals living in addictive family systems – obsession with controlling the thoughts, feelings and/or actions of others, lack of adequate or healthy psychological, emotional and physical boundaries in relationships, and inability to trust others. Certainly, one theme for individuals with high FAM scores involves their sense of happiness and self-worth being dependent on fixing or controlling the behavior of others. Jim may have learned early on the false perception that the only way he can have a sense of well-being is when he is in complete control of his partner. This need often can result in the perpetration of violence in cases where poor interpersonal boundaries and lack of trust exist in a person with serious impulse control problems. Thus, like other perpetrators of domestic violence, Jim may feel enmeshed at every level with his partner, seemingly unable to restrain himself when he feels like he is losing control of his partner’s behavior.
To summarize, Jim’s profile is similar in many ways to that of other known perpetrators of domestic violence who have completed the SASSI. Although he is classified as having a low probability of a substance use disorder, his responses are characterized by a significant degree of defensiveness. This, along with other assessment evidence, increases the risk that he has minimized his alcohol and other drug problems and that the SASSI results of low probability of substance use disorder may be inaccurate. Jim does not recognize or accept responsibility for his own behavioral problems. Like other domestic violence offenders, he tends to focus almost exclusively on controlling his partner’s behavior as a way of achieving happiness and contentment in life. Jim’s family history of alcoholism is likely a significant contributor to his behavioral problems and also increases the risk that he may have, or may be developing, a substance-related disorder.
Ongoing assessment will be necessary to completely rule out the possibility of a substance use disorder. Because of the impact that most psychoactive substances tend to have on reducing impulse control, Jim’s risk for reoffending is greatly increased if he has a substance-related disorder that is left untreated. Collateral sources of information concerning Jim’s alcohol and drug history seem to indicate that his problems with alcohol and other drugs may be more serious than he is reporting on the SASSI. If further assessment results confirm a diagnosis of a substance use disorder, his treatment plan would need to include some form of addictions therapy. In addition, a no-use contract and regular toxicological screens could be useful ways to lower his risk of using and support a period of abstinence.
Jim’s defensiveness could be a serious barrier to engaging him in a therapeutic relationship, let alone making any significant progress in helping him to change any of his problematic behaviors. Establishing rapport and gaining Jim’s trust and confidence would be important steps in creating and maintaining a therapeutic alliance with him. Didactic, cognitively based educational approaches are often viewed by defensive clients as less intrusive and non-threatening. Initially, he may respond more favorably to presentations, films, books, etc., emphasizing the impact of addictions on the individual and their families. This may help to increase Jim’s awareness of his own misuse of substances and provide him with some insight into the dynamics of his own family’s behavior, including his alcoholic mother. Family involvement in his treatment may also be beneficial.
Referral to a practitioner or program that specializes in treating perpetrators of domestic violence should be strongly considered. Remember that Jim may have little or no awareness that he is responsible for his own violent behavior. His perceptions may be completely dominated by the belief that he has a right to behave in this manner with his partner. Such deeply ingrained patterns of thought and associated impulse control problems are often difficult for clients to begin to recognize, much less change. Support and process groups facilitated by behavioral health professionals trained in the treatment of domestic violence offenders are often an effective approach in helping perpetrators begin to acknowledge their behavioral problems and to effect some healthy changes.
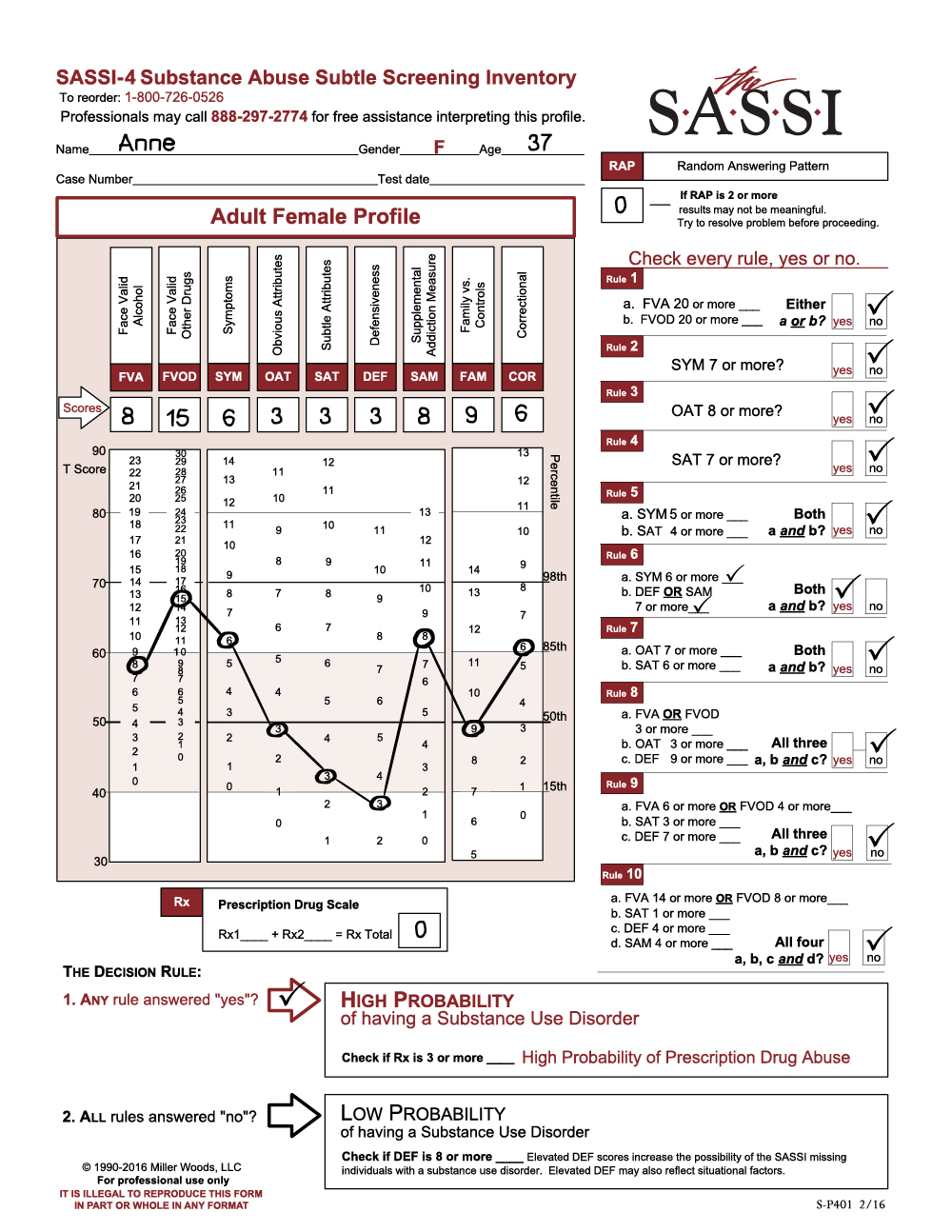
This SASSI-4 profile of a 37-year-old female was called in to our clinical support line. As we look at her results, it appears that she answered the items in a meaningful manner (RAP=0). She is likely to have a high probability of a substance use disorder (SYM=6, SAM=8) based on decision rule 6.
Notice that despite the relatively low DEF score and apparent lack of defensive responding, the SAM scale score, when combined with the elevated SYM score, leads to a test positive result. While it is true that the SAM scale score plays a vital role in the accuracy of the decision rules in this case, it is important to remember that the clinical meaning of this score is unclear. Therefore, it would be inappropriate to draw any clinical inference from the fact that the SAM score is elevated.
The client acknowledges significant problems related to her use of drugs other than alcohol. She is likely to have experienced some loss of control, negative consequences, and increased tolerance as a result of her substance misuse. However, her average OAT score (OAT=3) may be an indication of some limited ability or willingness to acknowledge behavioral problems commonly associated with individuals who have substance use disorders.
The moderately elevated SYM (SYM=6) is consistent with clients who often are not able to recognize the manner in which substance use is manifested in their lives. Her responses are similar to individuals who live in a social milieu where substance abuse and its related consequences are fairly routine and normalized. This experience may limit her ability to characterize her substance usage as problematic. Indeed, she may be somewhat surprised that the SASSI results could even indicate an addiction problem.
The client’s responses are similar to those of individuals who are experiencing emotional pain (DEF=3). Individuals who score in this range tend to be overly self-critical, may experience depressive symptoms and sometimes report a history of trauma. She may be quite limited in her ability to recognize personal strengths, focusing more on limitations, failures and feelings of low self-worth.
This client is likely to have a high probability of a substance use disorder and should be considered for relatively intensive addictions treatment. A comprehensive behavioral health evaluation may be necessary to rule out the need for additional psychiatric intervention. Although she demonstrates some ability to acknowledge relevant behavioral symptoms of her addiction, a viable treatment plan should include initial efforts to increase her self-awareness and insight into the full nature of her substance use problems. Education and other cognitively based interventions may be helpful.
Most likely, she will need help in recognizing that her misuse of alcohol and other drugs is similar to that of other substance dependent people. A content analysis of her responses on the FVOD and SYM items may be one way to help her realize that it is in her best interest and within her capacity to change.
Community-based self-help support groups could provide additional encouragement and support.
In addition, evaluation for depressive symptoms and its relationship to her substance us would be important to consider.
We had the opportunity
to consult with a treatment provider who had called in SASSI-4 scores for a
Native American couple residing in Canada. Since both profiles nicely
illustrate important clinical features of each client, we decided to present
the interpretations in this sample. We are grateful to the treatment agency in
Northern Canada that granted us permission to use the information included in this
sample. To facilitate the presentation of the profiles in a confidential
manner, we have created fictitious names for each of the clients.
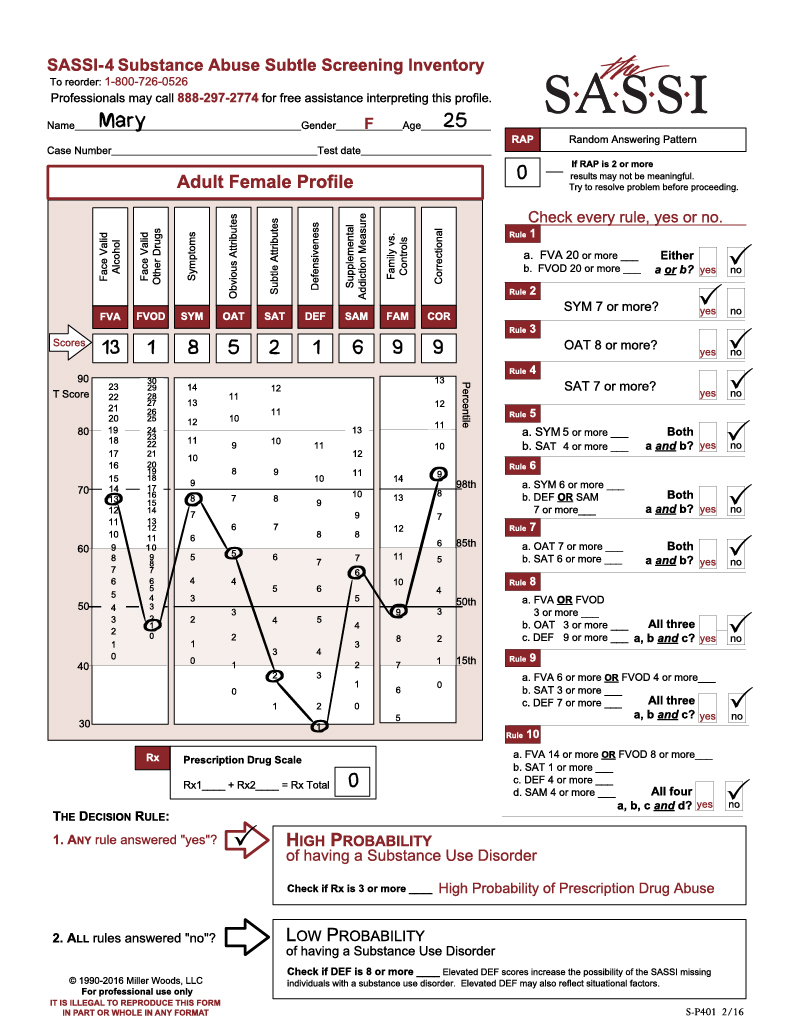
Mary, a 25-year-old
Native American female, and her husband John, a 28-year-old Native American
male, were referred to the agency for a substance use evaluation. They live in a
very small community where the base rate of substance misuse is extremely high.
Their children were recently removed from the home as child protective services
suspected alcohol abuse to be a serious problem for both parents. Mary lost her
mother, father and siblings in a tragic accident that occurred just a few
months prior to the evaluation.
Upon first glance at
Mary’s profile, she appears to have responded in a meaningful manner (RAP=0),
and there is no evidence of defensive responding (DEF=1). Given this low DEF
score, she is likely to be in considerable emotional pain. She acknowledges
significant problematic use of alcohol over her lifetime (FVA=13) and reports
behaviors and experiences that are highly correlated with substance abuse SYM=8).
In fact, her SYM score is the sole basis for classifying her as test positive
on the SASSI-4 (Decision Rule 2).
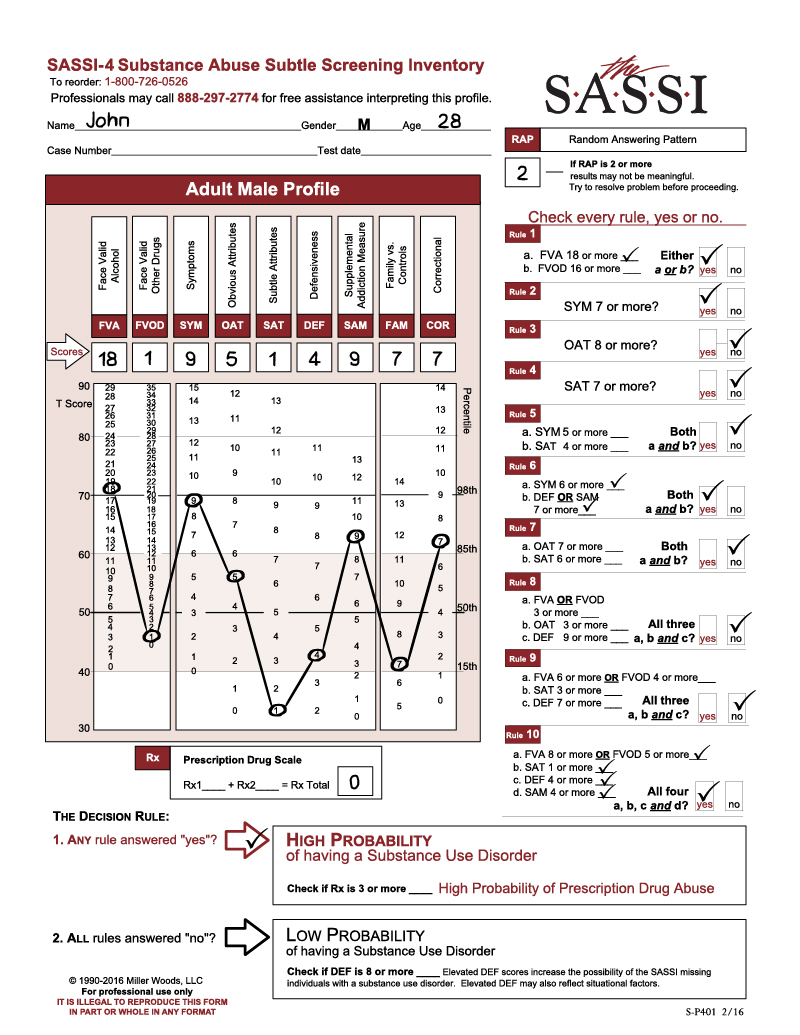
A quick look at John’s
SASSI results reveals a similar profile but with some noteworthy differences.
Although he too shows no evidence of defensive responding (DEF=4), his RAP
score of 2 raises immediate concerns of random or non-meaningful responding.
Fortunately, the treatment provider had investigated this potential problem and
was satisfied that John fully understood the items and that he responded in a
meaningful manner. The counselor attributed the elevated RAP to cultural
differences and circumstances surrounding the nature of the evaluation.
John also acknowledges
significant alcohol problems (FVA=18, decision rules 1, 2, 6, 10). Like Mary,
his responses are highly similar to individuals with substance use disorders
who report life circumstances and experiences commonly associated with substance
abuse (SYM=9). This score likewise results in a test positive on the SASSI-4 (Decision
Rule 2).
Having established
that Mary and John both have a high probability of a substance use disorder, we
can now proceed to examine the salient clinical aspects of the SASSI results,
hopefully illuminating more specific treatment needs for each client. Notice
that Mary’s and John’s SYM scores are highly consistent with the milieu in
which they are reported to have lived. The treatment provider made specific reference
to the high rate of alcoholism in their community. Individuals who have substance
use disorders with high SYM scores frequently live in environments where the abuse
of alcohol and/or other drugs and the associated consequences are common and
normal experiences. In fact, it can be such an accepted way of living in the
community that most of its inhabitants would be flabbergasted to have their drinking
behavior characterized as unhealthy or problematic. Consequently, it is
perfectly understandable that Mary and John may have difficulty recognizing the
precarious nature of their alcohol misuse, especially as it relates to their
current difficulties with the child protective agency.
Despite the similarity
of the two profiles, one important difference is Mary’s significantly low DEF
score. This score would certainly seem to fit in with the recent trauma she
experienced. Unresolved loss and grief issues may be strong contributing
factors to Mary’s emotional pain. Moreover, the thought of now losing her
children because of her substance use may be adding significantly to her
distress. The risk of depressive symptoms possibly related to a mood disorder
may indicate the need for a comprehensive mental health evaluation, especially
to rule out clinical depression or suicidal ideation.
Individuals with this
high a level of emotional distress are often overly self-critical and can
become immobilized with feelings of helplessness and hopelessness. However,
it’s also possible that Mary’s pain may act as a catalyst in helping her
recognize the need to do something about her drinking. Indeed, the treatment
provider confirmed this to be the case and described Mary as a willing
candidate for substance use disorder treatment.
On the other hand,
John’s focus may be less internally directed with a tendency to see people,
places or things outside himself as the major cause for his problems.
Individuals with low SAT scores often present as victims of circumstances,
powerless to change their behavior because of a perceived lack of influence and
control over their immediate environment. In John’s case, the treatment
provider reported that John perceived his wife as the major cause of his
problems. He was content to focus on Mary’s drinking, grief issues, and
possible infidelity as the sole source of difficulties in the family. Despite
his acknowledgment of significant symptoms related to his drinking (FVA=18
& SYM =9), he remained unwilling and unable to accept this as an important
causal factor.
A viable treatment
plan for this couple will have to take into consideration a number of issues.
Mary seems primed for substance use treatment but may need additional
behavioral health services. A comprehensive mental health evaluation would be
helpful in identifying the nature and extent of any concurrent problems.
Interventions directed at processing loss and grief and those that provide
support would undoubtedly be important actions to consider. Efforts should be
made to provide bonding opportunities with a treatment provider and other
sources of encouragement and affirmation. In this regard, community self-help
support groups would be a valuable adjunct to relatively intensive substance
use disorder treatment. Pending the results of the mental health evaluation,
additional behavioral health care services may be added as required.
Although John is also
in need of substance use disorder treatment, he does not appear to be a willing
candidate at this time. Efforts should be made to increase awareness and
understanding of his alcoholism and how it contributes to his relationship and
family problems. The SASSI-4 results could be used as a graphic illustration of
the serious nature of his drinking problems. Using the high SYM score, the
treatment provider may be able to convey some understanding of how John may
have difficulty seeing the unhealthiness of his drinking. A content analysis of
the FVA and SYM scales may help him to see specific ways in which his alcohol
misuse has affected his life. It would be important to keep John focused on his
own needs by helping him to accept responsibility for his life and to make
choices that are in his own best interest. Attendance at self-help support
group meetings could help to reinforce this notion. Conjoint or family therapy
may need to be deferred in order to reinforce self-focus and to discourage John
from externalizing blame to Mary.
This case emphasizes
the importance of recognizing and assessing the impact of environmental factors
when developing effective treatment planning. It is true that substance
dependent individuals often live in an environment where the abuse of alcohol
and other drugs is commonly practiced and accepted as a normal way of life. In
these situations, individuals frequently engage in heavy substance usage as a
means of maintaining acceptance and approval in the community. It’s no wonder, then,
that clients living in this type of environment are amazed when we begin to
identify their misuse of alcohol or other drugs as problematic. Given their
life experience, it would never have occurred to these clients that anyone
would view their drinking or drugging as a sign of serious problems.
As we were able to see from the above discussion, the SYM scale on the SASSI-4 can often help you to recognize this phenomenon as a potential issue to explore further. In cases where the SYM is significantly elevated, clients may express puzzlement and surprise at your suggestion that their substance use is contributing significantly to their problems. However, the knowledge that this reaction most likely stems from the normalization of substance abuse in a client’s milieu provides an opportunity for you to communicate empathetic understanding and develop further rapport with the client. Once an appropriate bond is established, efforts should be directed at helping the client achieve some awareness of and insight into the full nature of his/her substance misuse and its relationship to other presenting problems.