We wanted to let you know that we are still offering our free one-hour online Clinical Q&A sessions hosted by our Clinical Director, Kristin Kimmell, LCSW, LCAC.
We enjoy hearing how you are using the SASSI in your clinical practice and agencies as well as answering your questions. We currently have three more free Q&As coming up this year. You can reserve your spot and view available dates and times by clicking here. If you have profiles you would like to share with the group for discussion, please send them (de-identified) via email any time prior to the session to scarlett@sassi.com. Your contributions would be of great value.
Also, a reminder that we have a live certified SASSI training webinar on Administration & Scoring of the paper & pencil version of the SASSI on November 28th and Clinical Interpretation on December 5th. You can register by clicking here.
Note that the Q&A sessions do not provide CEUs and are not a substitute for SASSI Training. SASSI training provides 3.5 NAADAC CEs per session.
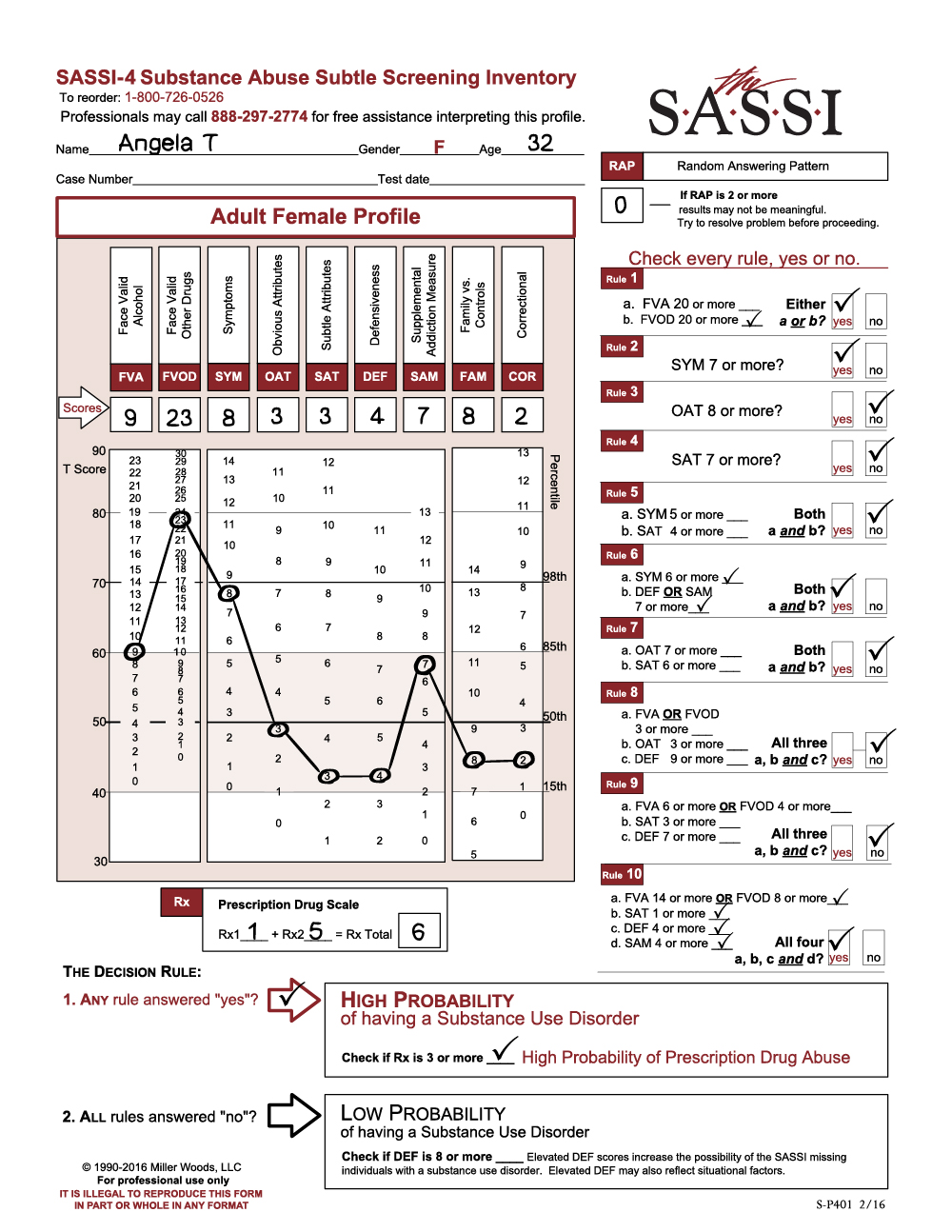
Angela T. illustrates a profile often seen in people who acknowledge that they use drugs excessively and have come to rely on them as a coping resource.
Angela’s scores on the SASSI-4 meet the criteria for classifying her as having a high probability of a substance use disorder. Angela’s score on the Rx scale also indicates a high probability of prescription drug abuse.
Reviewing her scale scores reveals openness in disclosing her use of drugs and alcohol. On FVOD and SYM, Angela acknowledges extensive use of drugs and many negative consequences and symptoms of abuse. Examining her answers to specific items on these scales may help you counsel Angela, and may suggest good starting points for a more detailed history of her use of alcohol, drugs and prescription medications.
On SYM Angela acknowledges serious substance misuse that she acknowledges resulted in making her problems worse, increased tolerance, excessive use, and wishing she could cut down her use of substances. Her OAT score is in the average range, which can indicate that Angela does not necessarily align herself with those characteristics associated with substance abusers and she may not see herself as a ‘drug addict.’
With her Prescription Drug scale (Rx) score of 6, it is useful to look at those individual items as well.
Angela’s moderate DEF score suggests she can be open and realistic in acknowledging her difficulties and substance misuse. The rest of her scores fall within the normal range, between the 15th and 85th percentiles.
Given Angela’s high level of drug use and consequences, you might consider a more comprehensive evaluation to determine whether she can maintain sobriety and function well enough to benefit from a treatment program. She may need supervised detoxification or other intensive intervention.
You may find Angela able to acknowledge that she uses drugs frequently and perhaps that she drinks to excess. However, she may not see that her behavior varies dramatically from others who don’t have a substance use disorder. Feedback on where her scores fall on the profile sheet may help her see that her behaviors are not typical. Examining the items that Angela endorsed on the FVA, FVOD, SYM, and Rx scales may provide useful insight into her motivations for using and help her see the consequences that result from her use. Angela may need your help to acknowledge her pain and to recognize that there are alternatives to her current lifestyle.
The SASSI-4 screens for Substance Use Disorder (SUD) along the full DSM-5 continuum of severity: mild, moderate, and severe. A brief scale, Prescription Drug (Rx), was added to accurately identify individuals likely to be abusing prescription medications. Read a full sample assessment report on Angela T. in the SASSI-4 User Guide & Manual.
The Substance Abuse Subtle Screening Inventory (SASSI) has been used successfully in correctional screening in multiple settings since its release. These include outpatient evaluations of offenders as well as assessments of incarcerated individuals in federal, state, and local correctional centers.
Many clients served in behavioral health and substance abuse treatment programs have histories of involvement with the criminal justice system in addition to mental health and substance use disorders. Samples in the SASSI-4 validation study included assessments in community corrections, probation and parole and drug courts, as well as cases from DWI and DOT education and screening programs. SASSI-4 overall screening accuracy in criminal justice settings was 95%; in DWI and DOT education programs SUD screening accuracy was 91%, and these accuracy levels were found not to differ significantly from the overall accuracy rate for all settings (92%). In addition, many cases included routine information on clients’ number and types of arrests and blood alcohol levels. Analyses revealed that SASSI-4 screening accuracy was 92% for clients with a history of criminal offenses, and 90% for clients who had no such histories.[i]
Interestingly, of those who had been diagnosed with a substance use disorder, criminal offenders acknowledged significantly less illicit drug use and consequences as well as less alcohol use and consequences on the SASSI-4 face valid scales than did clients with diagnosed substance use disorders in settings other than criminal justice programs — suggesting offenders minimized reported use and substance-related problems. By contrast, offenders with substance use disorders showed no differences in their endorsements of subtle items on the SASSI-4 compared to individuals with substance use disorders in other types of assessment settings. Despite offenders’ attempts at minimization, SASSI-4 overall accuracy in the offender samples was 94%. Together these findings illustrate strengths of using SASSI-4 to screen criminal offenders as compared to entirely face valid screens such as the AUDIT, CAGE or DAST. That is, the inclusion of subtle items on the SASSI-4 as well as a scale to identify clients’ level of defensive responding strengthens the ability of the SASSI-4 to accurately identify clients with substance use disorders.
In addition to legal offenses and possible substance use disorders, offenders also often have other mental health problems, which can affect their responses on many types of assessments they are given. Research on the SASSI-4 has shown its screening sensitivity is 98% in dual diagnosis clients; specificity is 93% in persons diagnosed with nonsubstance-related psychological disorders only, for an overall accuracy rate of 97% in people suffering from other psychological disorders. Moreover, accuracy was shown to be unaffected by ethnic background, and other demographic variables such as age and education.
For information on integrating the SASSI-4 into correctional programs, contact us at 800.726.0526.
[i] For additional validation information please refer to: Lazowski, L.E. (2016). Estimates of the reliability and criterion validity of the Adult SASSI-4. Springville, IN: The SASSI Institute.
Through the years, we have had the opportunity to share inspirational stories with our colleagues about their experience using the SASSI. One such story came recently from a psychologist who uses the SASSI in his practice. This was a gratifying story for us to hear and we are pleased that he has allowed us to share it with you.
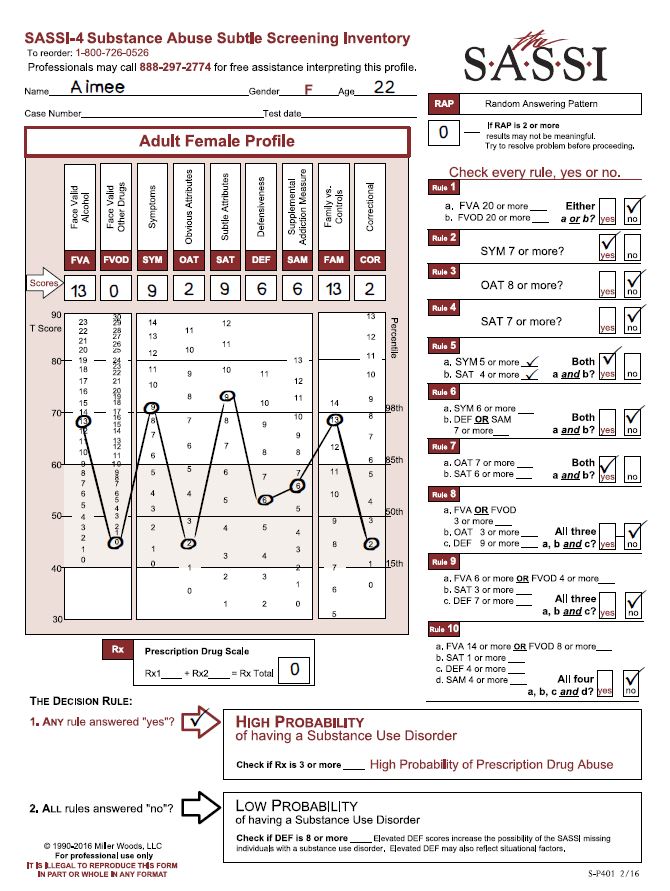
The mother of a 22-year-old woman called me because she felt very strongly that her daughter Aimee (not client’s actual name) had an alcohol problem. But Aimee was adamant, no question about it, “I don’t have a problem.”
After some persuasion, Aimee agreed to come into my office, and I invited her mother to stay in the office during the interview, with Aimee’s permission. I really think Aimee was very certain that there wasn’t a problem, and that having Mom there during the process would convince her mother of this, too. I said, “You know, Mom can be a bit of a reality check here, but I’m listening to what YOU are saying.” Aimee’s mother agreed to just listen, since she had had her say when making the referral.
We talked about it, and Aimee restated that she didn’t have a problem. She was just not aware of any bad consequences coming from drinking. Aimee really seemed to believe what she was saying, “My friends and I, we don’t have any consequences; we just enjoy drinking.” I told her that was fine and asked, “Would you like to find out if you, in fact, do have a problem, or would you rather not know?” Of course, this is right in front of Mom. And she thought about it, seeing herself as being free to say “no.” But she did say, “Yeah, I think I would want to know.” When asked about each of the DSM diagnostic criteria for substance use disorders, Aimee answered no to all symptom questions.
Then, I brought out the SASSI-4, and told her a little bit about how it would compare her responses to two known groups of people: those who have a problem and know it, own it, and the other group that is just as aware that they do not have a problem, and own that. And we will see how your responses go. She agreed that that sounded good. She took the SASSI-4, and her responses showed a high probability of having a substance use disorder. This was very surprising to her. Then I went back and showed Aimee her scores on the FVA and the SYM.
When she looked at those scores, she could see by the profile that the consequences she was getting were way out of line compared to ordinary people who drink. She runs with folks whose norm is to drink a lot, and there is a history in her family of substance use issues. She just said, “It’s almost like thinking about it and realizing that you are surrounded, and your best bet is to give up!” She surrendered to the idea that, “Yes, I’ve got a problem.” From there on she was willing to do something about it. Aimee made an appointment to see me again, and we went on from there.
Let’s say that the SASSI did not exist, and I would have had only the DSM criteria and her history. I would have had her mother’s reflections and thoughts and observations, and—I don’t feel certain, but I’m guessing—she would have walked away with the understanding that she did not have a problem. She would have gone on as she had been—because I would not have been able to make a case that she did have a problem, because there would have been no data to base that on. She may well have been one of those who left the interview, and for the rest of her life said, “No, I don’t have a problem, so get off my back.” In a sense, I really believe that the SASSI saved this young woman’s life, or at least spared her significant pain. I have always been impressed by the accuracy of the SASSI. It picks up on people who really are “sincerely deluded.” It’s interesting that her score on the Defensiveness (DEF) scale was not particularly elevated, so it was not that she was being defensive, she was just unaware of how her drinking and symptoms associated with it were beyond the norm. Her elevated SAT score – at the 98th percentile – supports the interpretation that Aimee has little insight into what may be motivating her to drink with her friends, or the negative consequences that follow from spending time that way. I am very grateful for the SASSI, and I wouldn’t do an assessment or a screening without it. I literally would refuse, because just the verbal reports can be so misleading, although not intentionally misleading, necessarily. Clients will compare themselves with the people they know who are much further along in the addiction process, and not really understand that their own behavior is a problem, just because their own behavior is not yet as severe as what they see in others. The SASSI can put a client’s use into a broader, and often more realistic context.
Original depiction, written by Nancy Winningham, M.A. based on an actual experience a clinician had using the SASSI with a client. Adapted to reflect SASSI-4 information.
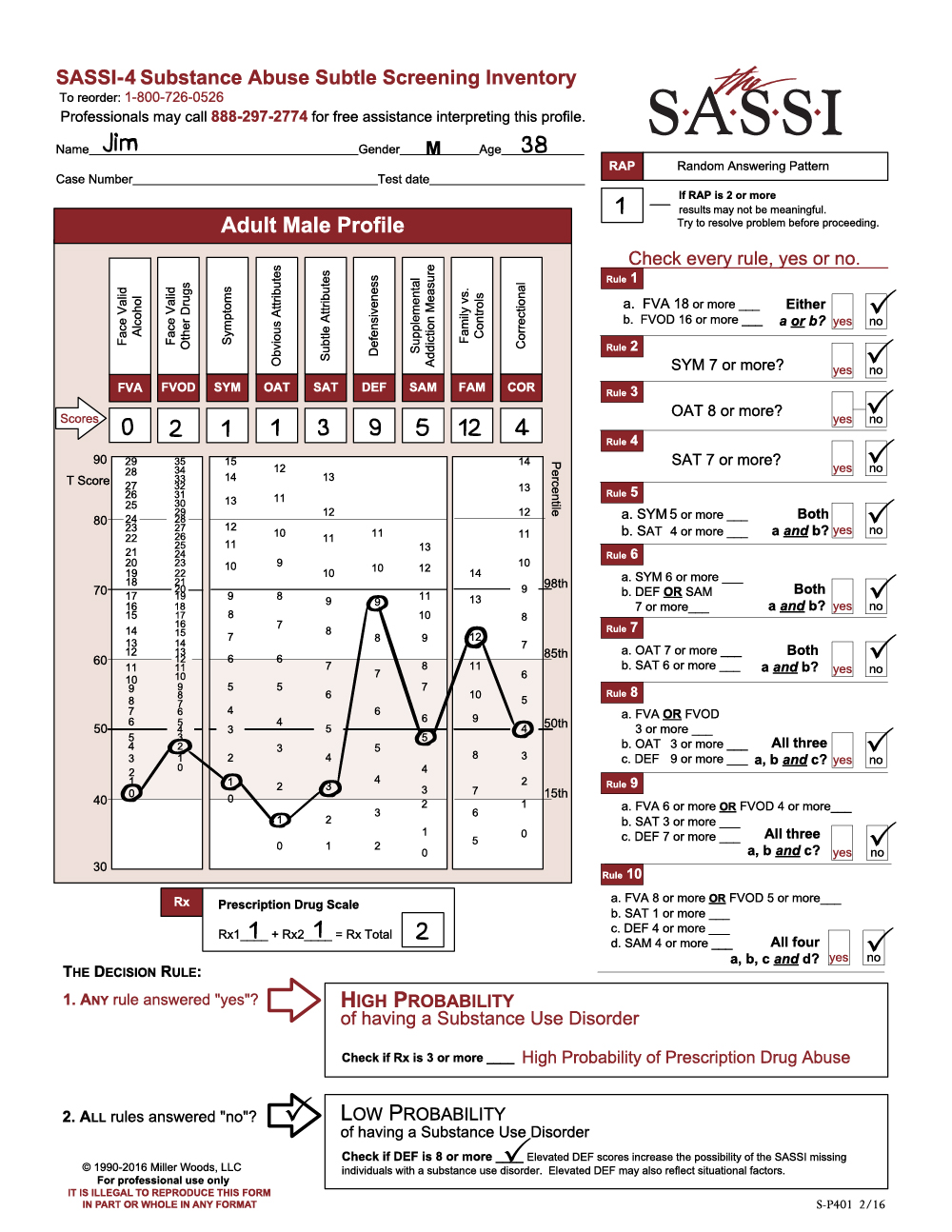
The client is a 38-year-old male named Jim (not his real name), who was referred for a substance use evaluation following a second arrest for domestic violence. The practitioner calling in the profile reported having collateral evidence substantiating a significant history of alcohol abuse for this client.
The SASSI results indicate that Jim has a low probability of having a substance use disorder. He is not acknowledging any significant problematic use of alcohol (FVA=0) or other drugs (FVOD=2). In fact, he denies having any of the symptoms commonly associated with individuals who have substance use disorders (SYM=1). However, note that Jim’s responses are highly defensive (DEF=9) and significantly similar to individuals who are instructed to minimize and conceal problems. Given that his report on the FVA and FVOD is in direct conflict with information from other sources, it is likely that he is minimizing the degree to which he has experienced alcohol and other drug problems or related symptoms. This increases the risk that the SASSI classification of low probability may be in error – in other words, the accuracy of the decision rules may be slightly decreased. As in most assessment situations where the client is relatively defensive, augmenting self-reported alcohol and drug history with data from external sources is advisable before ruling out substance use problems.
Experienced SASSI users working in criminal justice, EAP, DOT, child protection, and other similar settings will recognize this profile as relatively common for clients who are mandated for assessment. Indeed, Jim has been charged with assaulting his partner for a second time. One possibility is that he fears a harsh punishment may be coming if he does not present himself in a favorable way. He may also be convinced that he is not to blame for his behavior, explaining that his partner provoked him or that he was acting in self-defense. While the SASSI does not reveal the exact cause or reason, the high DEF score is a strong indicator that Jim approached the assessment in a defensive manner.
Notice also that Jim’s OAT score is significant given that it falls below the 15th percentile (OAT=1), meaning that only 15% of the general population would score this low. A score in this range usually indicates a person does not identify with any of the problematic behaviors typically associated with substance abuse (for example, anger management problems, negativity, self-centeredness, etc.). Jim is not likely to acknowledge having these behaviors and probably wants to be viewed as being completely different from people who do. Individuals with a family history of addictive or violent behavior often cope by distancing themselves from the addict or perpetrator as if to say, “I’m nothing at all like my alcoholic mother or physically abusive father.” In fact, the caller reported that Jim’s mother is an active alcoholic.
Jim’s FAM score of 12 is also significantly elevated (above the T 60 line or the 85th percentile). His responses are similar to family members of substance dependent individuals. It is likely that he shares many of the characteristics and traits commonly associated with individuals living in addictive family systems – obsession with controlling the thoughts, feelings and/or actions of others, lack of adequate or healthy psychological, emotional and physical boundaries in relationships, and inability to trust others. Certainly, one theme for individuals with high FAM scores involves their sense of happiness and self-worth being dependent on fixing or controlling the behavior of others. Jim may have learned early on the false perception that the only way he can have a sense of well-being is when he is in complete control of his partner. This need often can result in the perpetration of violence in cases where poor interpersonal boundaries and lack of trust exist in a person with serious impulse control problems. Thus, like other perpetrators of domestic violence, Jim may feel enmeshed at every level with his partner, seemingly unable to restrain himself when he feels like he is losing control of his partner’s behavior.
To summarize, Jim’s profile is similar in many ways to that of other known perpetrators of domestic violence who have completed the SASSI. Although he is classified as having a low probability of a substance use disorder, his responses are characterized by a significant degree of defensiveness. This, along with other assessment evidence, increases the risk that he has minimized his alcohol and other drug problems and that the SASSI results of low probability of substance use disorder may be inaccurate. Jim does not recognize or accept responsibility for his own behavioral problems. Like other domestic violence offenders, he tends to focus almost exclusively on controlling his partner’s behavior as a way of achieving happiness and contentment in life. Jim’s family history of alcoholism is likely a significant contributor to his behavioral problems and also increases the risk that he may have, or may be developing, a substance-related disorder.
Ongoing assessment will be necessary to completely rule out the possibility of a substance use disorder. Because of the impact that most psychoactive substances tend to have on reducing impulse control, Jim’s risk for reoffending is greatly increased if he has a substance-related disorder that is left untreated. Collateral sources of information concerning Jim’s alcohol and drug history seem to indicate that his problems with alcohol and other drugs may be more serious than he is reporting on the SASSI. If further assessment results confirm a diagnosis of a substance use disorder, his treatment plan would need to include some form of addictions therapy. In addition, a no-use contract and regular toxicological screens could be useful ways to lower his risk of using and support a period of abstinence.
Jim’s defensiveness could be a serious barrier to engaging him in a therapeutic relationship, let alone making any significant progress in helping him to change any of his problematic behaviors. Establishing rapport and gaining Jim’s trust and confidence would be important steps in creating and maintaining a therapeutic alliance with him. Didactic, cognitively based educational approaches are often viewed by defensive clients as less intrusive and non-threatening. Initially, he may respond more favorably to presentations, films, books, etc., emphasizing the impact of addictions on the individual and their families. This may help to increase Jim’s awareness of his own misuse of substances and provide him with some insight into the dynamics of his own family’s behavior, including his alcoholic mother. Family involvement in his treatment may also be beneficial.
Referral to a practitioner or program that specializes in treating perpetrators of domestic violence should be strongly considered. Remember that Jim may have little or no awareness that he is responsible for his own violent behavior. His perceptions may be completely dominated by the belief that he has a right to behave in this manner with his partner. Such deeply ingrained patterns of thought and associated impulse control problems are often difficult for clients to begin to recognize, much less change. Support and process groups facilitated by behavioral health professionals trained in the treatment of domestic violence offenders are often an effective approach in helping perpetrators begin to acknowledge their behavioral problems and to effect some healthy changes.