Alyssa (revised) is a 14-year-old female adolescent sent for evaluation by her teachers after noticing significant changes in her emotions and behavior. Her demeanor has gradually changed from a smiling, mostly compliant teen to that of a more rebellious and sullen one. She’s been caught skipping school a few times and was found to be in the company of some older adolescents who are consistently in trouble and suspected of using alcohol and drugs. The SASSI-A3 classified Alyssa with a LOW PROBABILITY of having a substance use disorder (SUD). Neither the VAL or DEF scale scores met the criteria for the possibility of a false negative. While the scale scores do not meet the criteria for classifying her as high probability of having an SUD, there are some other scale scores which could indicate some other clinical issues that may need to be addressed.
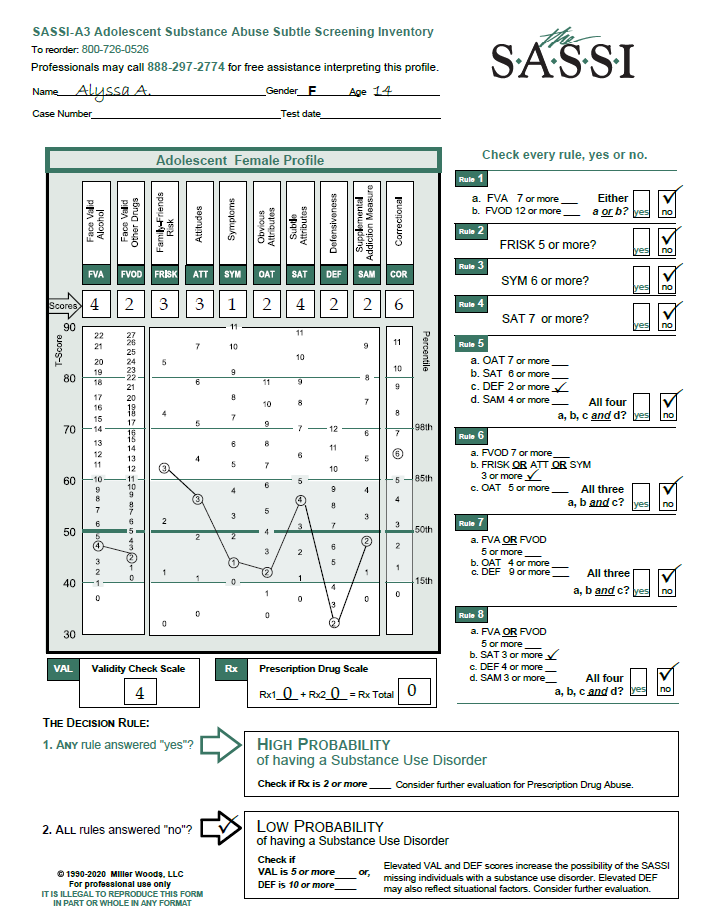
In going beyond the decision rules and looking at the individual raw scale scores, it is possible to develop a more general hypothesis regarding her level of adjustment and functioning. The fact that she scored above a zero (0) on the FVA, FVOD and SYM scales tells us that, while her scores are not high enough to indicate the probability of an SUD and are in fact very close to the mean, at 14 years old she has used both alcohol and drugs and experienced some negative consequences and/or problems as a result of that use. Based on her elevated FRISK score of 3, her slightly elevated ATT score of 3 and her elevated COR score of 6 (along with the observations made by her teachers), we can further hypothesize that Alyssa is likely to be surrounded by a close social system who are abusing substances and, as a result of this, her attitudes toward substance use lean more toward endorsing and promoting such use as a good thing. Assuming that this social system likely consists of her peers, namely the older teens mentioned earlier, this may explain her elevated COR scale score. In other words, she may have similar thinking patterns, beliefs, values and attitudes as those who are more likely to engage in rule-breaking, unlawful behaviors and/or disdain for authority. Her OAT score seems to indicate that Alyssa does not at all identify with any of the typical attributes that we would normally associate with an active substance abuser and that she firmly believes that she does not have a substance use problem. One of the most concerning scale scores on this profile is the DEF score of 2. SASSI research tells us that very low DEF scores such as this, often indicate a young woman who is experiencing a great deal of emotional pain and many of the typical symptoms associated with a syndrome of clinical depression. She may tend to engage in negative self-statements, identifying herself as a loser or misfit. She may be experiencing a sense of hopelessness, inability to enjoy positive experiences, lethargy, general bad feelings, impaired functioning in vital areas such as sleeping and eating, and sometimes even suicidal ideation.
While a low DEF score is not a clinical diagnosis in itself, this profile raises some questions that a counselor may wish to pursue in an interview or further ongoing assessment. For example, what is causing the significant change in emotion and behavior that was noticed by the teachers? Is it simply the normal emotional volatility of a growing and changing adolescent? Is there something happening in this teenager’s family which has caused this sudden shift in emotion and acting out? In any case, hopelessness, suicidal ideation, depressive symptoms or other psychiatric problems are important concerns to be investigated. It would also be valuable to explore the extent and context of her drinking and drug use to determine if it is just normal adolescent experimentation, a reaction to peer pressure, or an attempt to deal with emotions too overwhelming to control on her own. While the SASSI does not indicate a high probability of having an SUD currently, without some sort of intervention regarding these sudden changes in emotions and behaviors, a future SUD problem is not out of the question. It is difficult to suggest appropriate interventions without further information. However, appears that she could benefit from seeing a safe, trustworthy and empathetic counselor who could further explore the issues and immediately address her emotional pain and help her develop coping skills other than alcohol and/or drugs. Using the raw scale score interpretations described previously, in an open two-way conversation the therapist and Alyssa could use these scores to begin to collaboratively develop a plan of action that could help her confront and overcome the difficulties she is facing.
We hope you find this useful information regarding clinical issues. As always, the Clinical Helpline at 888-297-2774 is open to serve you Monday through Friday, 1 pm to 5 pm (EST).