If you have attended one of our trainings either in-person or online, you know the section on how to administer the SASSI to a client is one of the most important. A thoughtful approach can set the tone for the entire assessment by helping a client feel more at ease and engaged in the treatment process. We emphasize the importance of first establishing rapport with the client. The questionnaire is presented as an aid, not a test with right or wrong answers. We instruct to administer the true/false side first, then checking the appropriate time frame for the face valid side. Letting the client know s/he will have a chance to discuss the results at a later time increases the client’s comfort level.
Our protocol is based on the recommended one-on-one consultation. We realize that is not always possible. Administrators of the SASSI work in a variety of settings including schools, probation departments, EAP, treatment agencies, institutions and private practice. Since the SASSI does not require a professional to administer it, a variety of personnel can be trained, but both the context and the administrator can have a significant impact on the receptivity of the client.
This example of the context of a SASSI given to a client dramatically shows the difference the setting can make in the results. One of our clinicians fielded this call. The administrator did not know which results to use even though both profiles came up with a high probability of having a Substance Use Disorder.
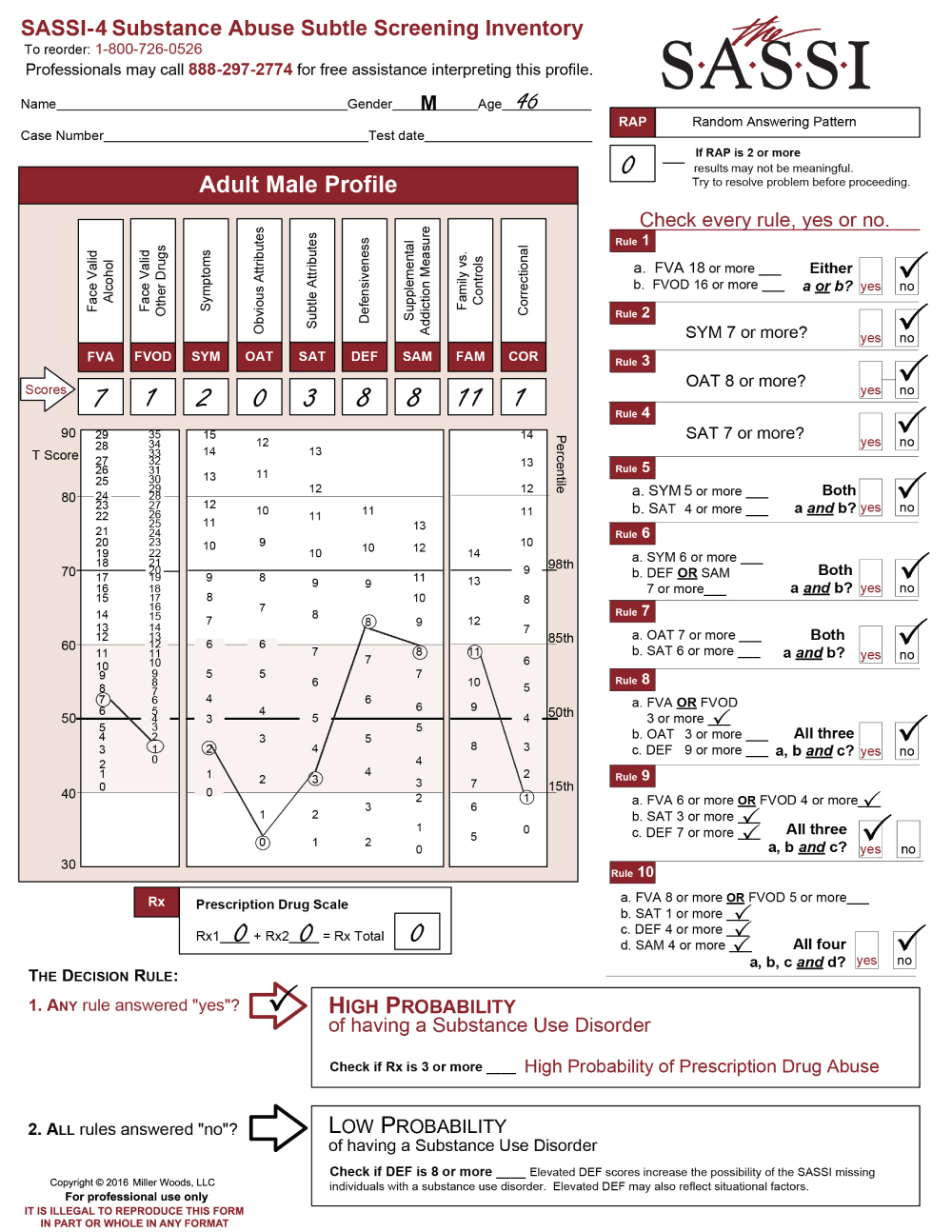
The client is a 46-year-old male who was given the SASSI at the Courthouse in a packet of material he was instructed to complete. Two weeks later he was given another SASSI to complete. This time with a counselor assigned to evaluate him.
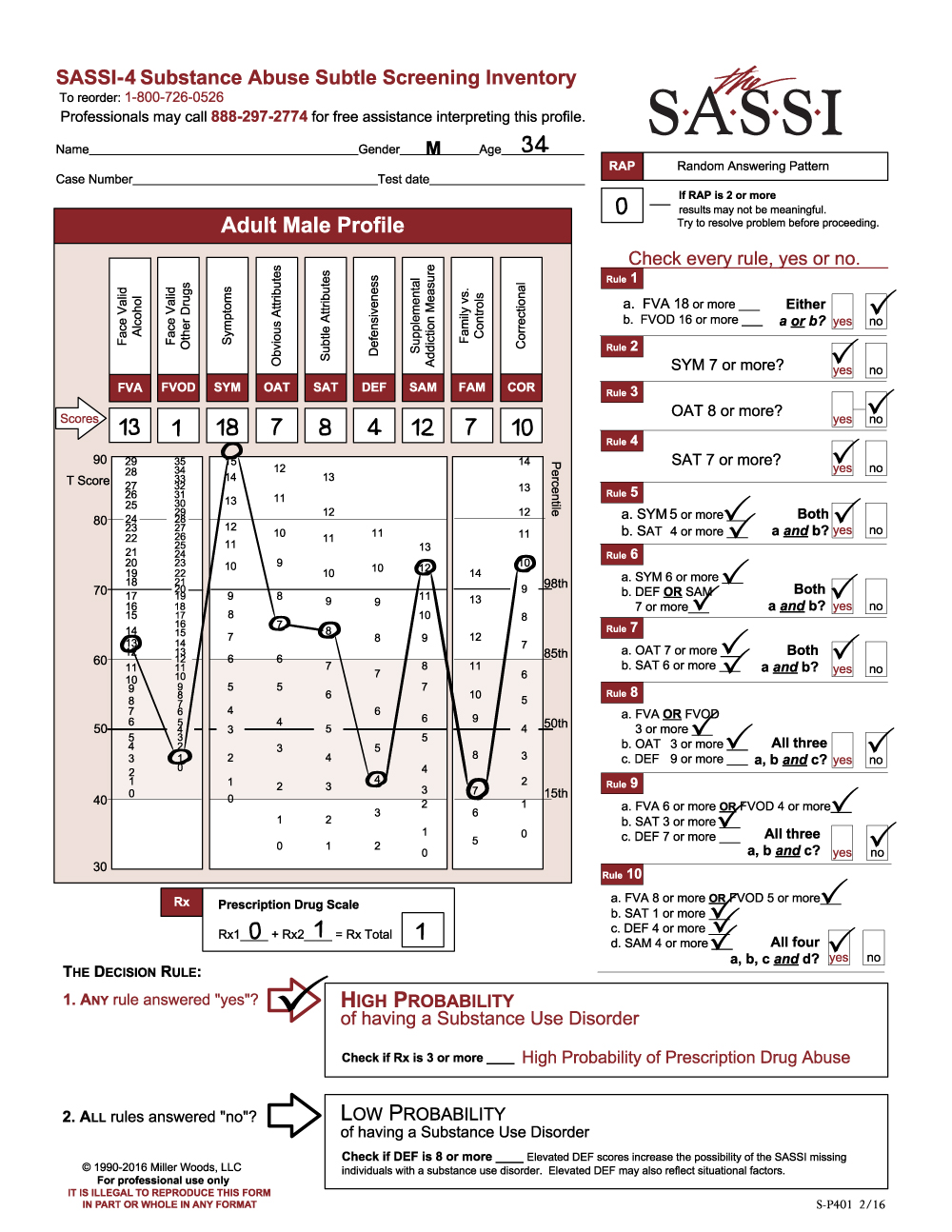
Here are the results of the first SASSI he completed at the Courthouse:
As you can see, he meets Decision Rule # 9. Looking at the graph, some scales and numbers stand out. On his face valid scales, including SYM, his numbers were within the norm, between the 15th and 85th percentile. His OAT score is extremely low which indicates he has a hard time acknowledging personal limitations or shortcomings and may have difficulty in groups. The other significant score is the DEF score of 8. In spite of the elevated DEF score, he did meet one rule. The SAM is almost at the 85th percentile so, in my mind, I might be more inclined to say he was defensive about his substance use and perhaps minimizing on the face valid scales. This hypothesis would depend on the rest of the assessment with any additional information. However, he was given the SASSI to complete within a packet of materials, and it is very unclear what instructions he was given, if any, on how to complete the SASSI.
Let’s look at the results of the 2nd administration given just two weeks later in the office of the counselor who was evaluating him after meeting and talking with the counselor.
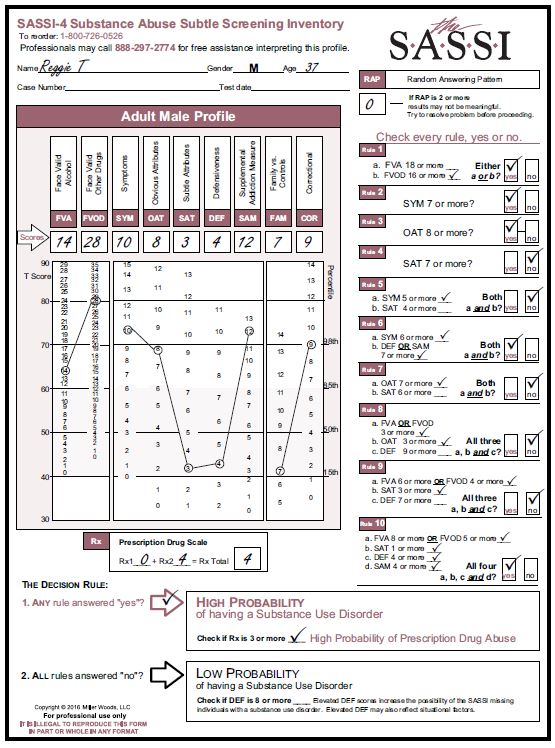
In this profile, the client meets multiple decision rules including numbers 3, 4, 5, 6, 7 and 10. All it takes is one rule to meet high probability and more than one does not mean a more severe substance use disorder. Diagnosis and severity are based on the DSM-5 criteria. It is evident his raw scores have changed to impact the decision rule results.
There is a significant change in his Face Valid Scales with an FVA of 11 and an FVOD of 14. His SYM score of 6 also shows elevation. OAT has changed from a 0 to a 9. He is now indicating a willingness to acknowledge shortcomings and limitations. In addition, he probably can identify with other substance abusers so a referral to a group treatment program can be considered.
The significant drop in the DEF score from an 8 to a 5 is nice to see. The client met with the counselor who was able to establish rapport by making the client more comfortable and explaining what the SASSI is and how it will be used in the context of the assessment. The low FAM score reflects the client’s internal state of mind. He is probably very concerned about what is going on within himself and not so concerned about others.
The final interesting scale change is the COR score and probably more representative of the client’s self- assessment at this point. Perhaps he is more able to identify impulsive or anger management issues, risk-taking behaviors, low frustration issues, or poor social skills. It gives the counselor some insight on what to explore, regarding behaviors which are impacting the client’s choices.
The most important difference in these two profiles was how the SASSI was presented to the client. Context, and establishing rapport can produce a more useful SASSI by obtaining a depth of clinical information. As an aside, we were not informed on why the SASSI was administered twice within a two-week time frame. We do not usually recommend doing so. It may have been the counselor was unaware of the first SASSI administration until receiving the completed materials from probation.
We hope you find this useful information regarding clinical issues. As always, the Clinical Helpline at 888-297-2774 is open to serve you Monday through Friday, 9 am to 5 pm (EST).
PDF Version Available for Download