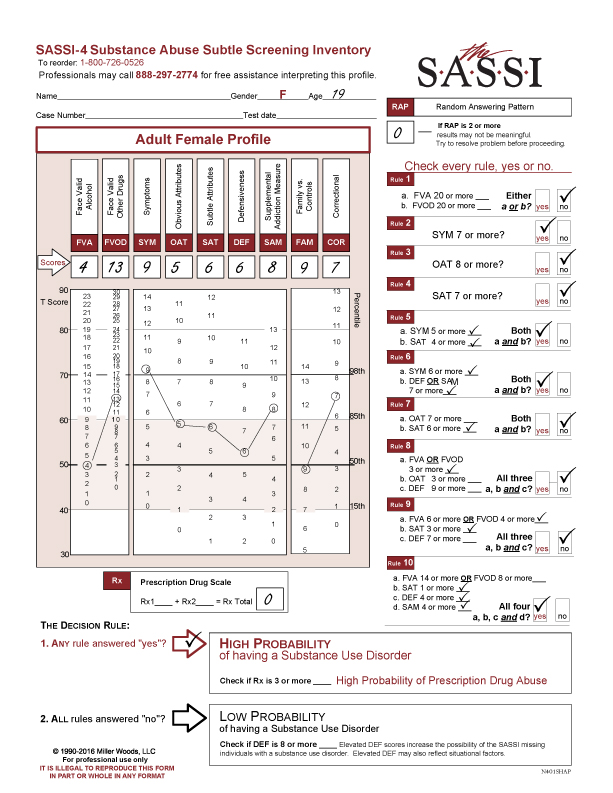
This profile is a good example of needing to be careful with assumptions.
Overview of CORRECTIONAL (COR) SCALE
The COR scale provides information pertaining to the possibility that the client may have a relatively high risk of experiencing legal problems. It is composed of items that differentiated between people who had a history of involvement in the juvenile justice system and those who did not.
It is very important not to over-interpret elevated COR scores. Teens who have elevated COR scores are responding similarly to individuals who have violated the law. This does not mean that all clients with elevated COR scores have broken laws. Also, there is no empirical evidence that these clients are at risk for future offenses.
If a client has an elevated COR score, it is worth exploring those behaviors which may be leading the client to make poor choices, especially after using substances and magnifying the tendency to exhibit those behaviors. These include anger management issues, impulsivity, risk taking behaviors, low frustration tolerance or poor social skills. The task of the clinician is to help the client see the relationship of their behavior to the consequences they have experienced and introduce alternatives to regulate their emotions and behavior.
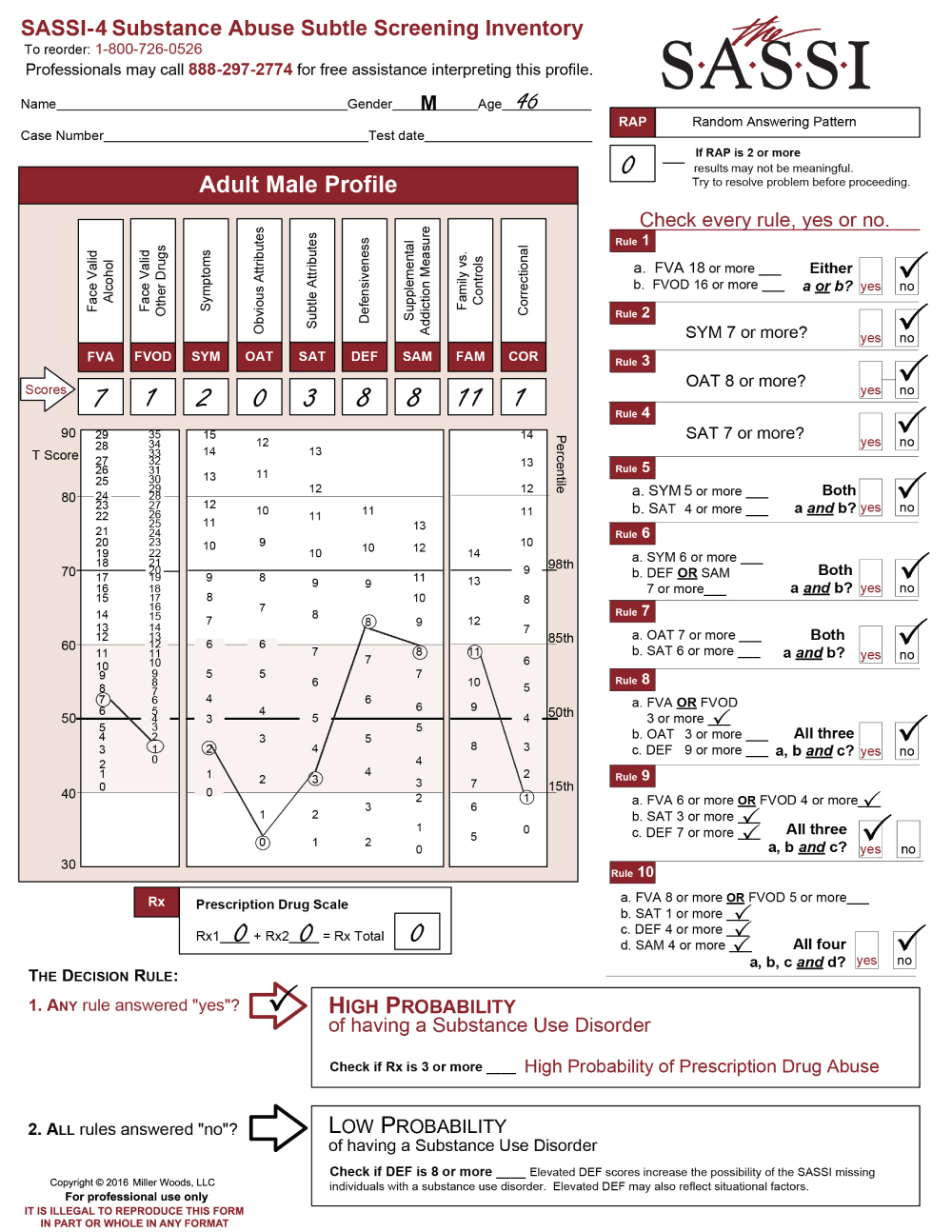
The SASSI A3 was administered on a 15-year-old male and the time frame for the FVA/FVOD was for the past 6 months. The caller explained this time frame was used as the client identified that his substance use became problematic during this time. He indicated he had initially started smoking marijuana but in the last 6 months started abusing Percocet.
There is a lot to look at in this profile below.
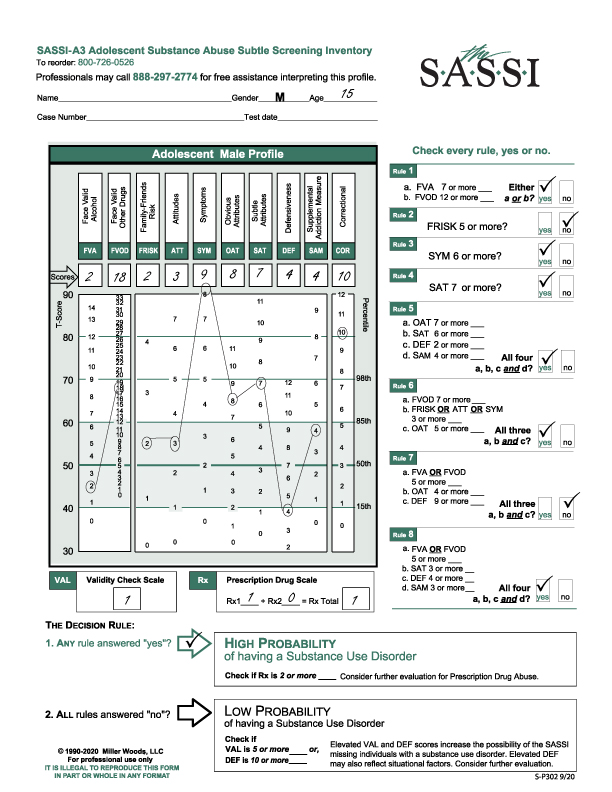
He meets Rules 1, 3, 4, 5, 6 and 8 so met the criteria of a High Probability of having a Substance Use Disorder. A reminder that more “yeses” does not necessarily mean a more severe problem or meets the DSM-5 criteria for severity.
His Rx scale score was 1.
The FVA (2) is below average and within the norm.
The FVOD (18) is highly elevated and close to the 98th percentile so he is very open about his use and under what circumstances he is using.
As seen on the profile graph, both the FRISK (2) and ATT (3) are within the norm though above average. These scores indicate he is not necessarily using due to peer pressure nor does he have a strong belief or value system that endorses substance use.
The SYM (9) is off the chart. He is endorsing negative consequences and symptoms of his use as well as loss of control.
It is worth taking the time to look at how he has answered his face valid scales and do content analysis of his answers because these will generate a lot of information for clinical insight and discussion on how and why he is using substances. As a reminder, the face valid scales are the FVA, FVOD, FRISK, ATT, SYM and Rx scales. You cannot do content analysis on the subtle scales.
Both the OAT (8) and SAT (7) are above the 85th percentile. Although the OAT indicates he can acknowledge personal limitations, the higher SAT score indicates a level of denial or lack of awareness or detachment from feelings and may present himself functioning well.
The DEF (4) score is very significant as it is below the 15th percentile. This indicates severe emotional pain, and he may be exhibiting depressive symptoms so it is suggested a mental status exam should be conducted.
As usual, there is no individual clinical interpretation to SAM (4).
The last scale, COR (10) is highly elevated above the 98th percentile. He is identifying with those issues that are normally seen in juveniles with legal issues.
This is where one must be careful with assumptions because this client has had no legal issues for any reason. It is more productive to explore those issues he is identifying with and affecting his choice making.
It is also curious that one can be very open (based on the FVOD and SYM) yet have an elevated SAT score as well. This may be due to the DEF score and the emotional pain he is in. Hypothetically, he may believe that if he was not “depressed” he would not be abusing drugs.
Another aspect of the profile is to explore his Rx result. According to the client’s report, he is primarily abusing Percocet. His score may reflect he is getting it illicitly and not through a doctor.
Finally, regarding treatment considerations, the caller reported he has tried to quit using the Percocet for a week but relapsed. A treatment plan including inpatient should be considered considering his reported relapse.
We hope this is helpful to you.
The clinical helpline line is open for your inquiries, M-F, 12- 5 (EST) at 888-297-2774 and you will be directed to a clinical consultant. If we are not available, please leave a message and we will return your call.
And as always, Thank you for your interest in the SASSI.