The message this Adolescent was trying to send is as confused as he must be. A lot of contradictions in the numbers needed to be sorted out and made sense of.
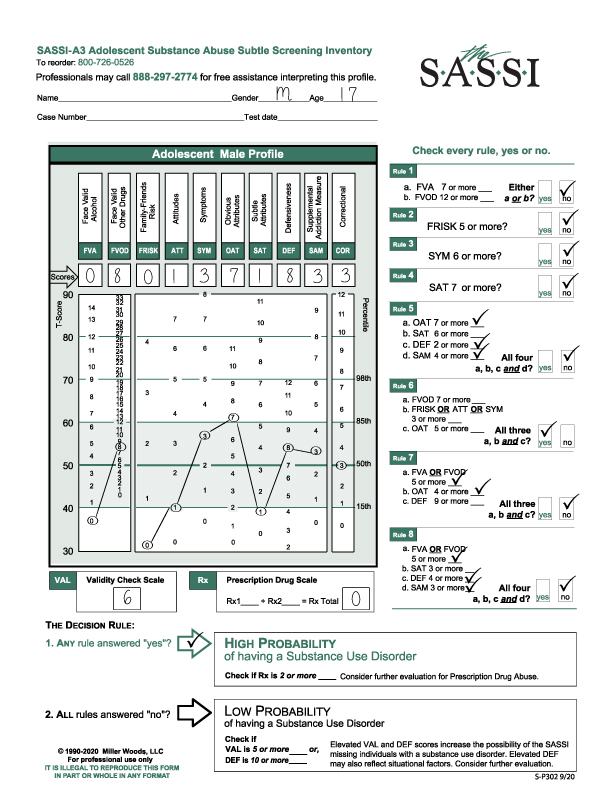
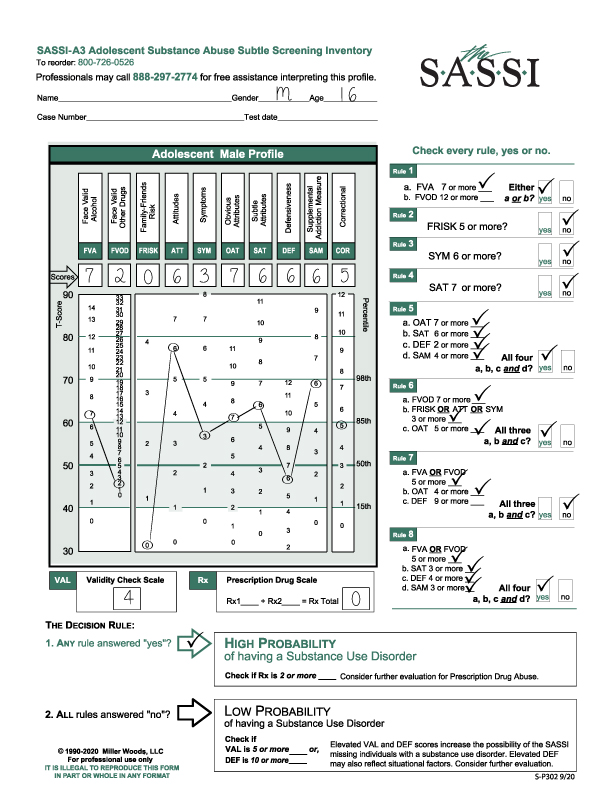
This 16-year-old male responded to the FVA and FVOD questions for his whole lifetime.
The Prescription Drug Scale result was zero.
The VAL check was 4.
He met the criteria for a High Probability of a Substance Use Disorder based on Rules 1, 5, 6 and 7. A reminder, it requires only 1 yes to the 8 rules to meet the criteria for High Probability. More “yes’s” does not mean a more severe problem. Severity of a Substance Use Disorder is determined with a diagnosis from the DSM-5.
Another reminder, content analysis of the Face Valid scales i.e. FVA, FVOD, FRISK, ATT, SYM and Rx individual items can be examined to generate information regarding under what circumstances substances are used and with whom, along with underlying emotional reasons.
The FVA of 7 is elevated enough to meet the criteria of Rule 1. The FVOD of 2 is below average and within the norm.
The FRISK score of 0 proves to be interesting given the context of the psychosocial history of this individual. It may be he did not want to disclose information regarding his friends or family.
The ATT score of 6 is highly elevated above the 98th percentile. This indicates he has a strong value and belief system regarding the use of substances. He may believe that everyone uses and that may be the case in his world.
The SYM score of 3 is within the norm so from his perspective, he has experienced minimal symptoms or consequences of his usage.
The OAT score of 7 is elevated above the 85th percentile so clinically significant but coupled with an higher SAT score of 6 as graphed is somewhat muted. On the one hand, an elevated OAT score indicates he can acknowledge personal limitations and shortcomings and may identify with other substance users though he may not want to change. On the other hand, the elevated SAT score can indicate denial or lack of awareness and insight or detachment from feelings.
The DEF score of 6 is within the norm and below average which can indicate self-esteem issues. It is a bit surprising the DEF score, in this case, is not elevated. The client was not defensive completing this questionnaire.
The SAM score, by itself, has no clinical interpretation.
The COR score of 5 is within the norm so there is no clinical interpretation.
What the psychosocial interview revealed: The client had a history of vaping nicotine with friends and had completed a Substance Use Education course. However, the client was smoking pot at home and minimizing his use. He was described as lying and manipulative. It was also disclosed his father is in recovery. As we all know, attitudes around Marijuana not being addictive or even a “drug” have been rapidly changing along with the legalization of Marijuana. However, the client’s risk of developing a significant risk of a substance use disorder is escalated by a family history of addiction.
Addressing the VAL score of 4: With the High Probability of a Substance Use Disorder result, the VAL check score does NOT come into play. It would only be impactful if he had come up with a LOW Probability of a SUD. However, this score is quite high, and the administrator would rightly suspect the client was trying to skew the results even if it had no impact on the result.