
A substance use evaluation administered on an individual involved in a custody suit can reliably be fraught with issues. This one presents a number of them.
This 39-year-old client was instructed to complete the FVA/FVOD questions for his whole lifetime.
A significant issue was his history of 4 DUI’s from 2020 – 2021 while in the process of separation and divorce. He denies his current use is anything like it was during that period.
The SASSI result indicated a Low Probability of a substance use disorder.
His RAP was 1 but not enough to flag the results and his Prescription Drug Scale was zero.
Looking at how his scores compare on the graph; we first see the average scores of his FVA and FVOD scales which may be suspect given his DUI history. His average SYM score suggests he does not acknowledge significant symptoms or consequences of his use despite 4 DUI’s. Face Valid Scales are easy to manipulate or minimize if the client chooses as they directly relate to substance use.
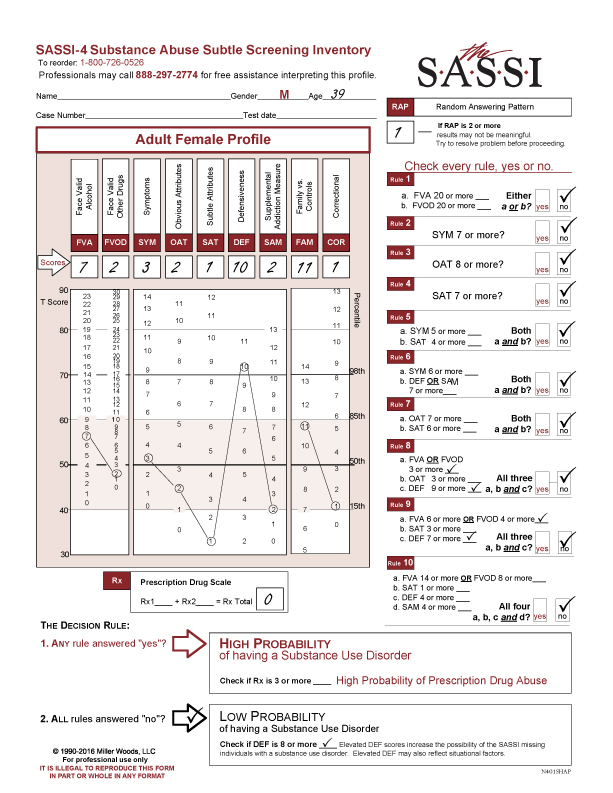
Moving on to the subtle scales starting with OAT, we see it is very low but within the norm. If it were any lower, it would indicate he has a hard time acknowledging personal limitations and shortcomings so there may be a hint of that going on. It is the next two subtle scales which contribute the most. The SAT scale is below the 15th percentile and when it is this low can indicate the client is hypersensitive to what others think of him, maybe experiences feelings of rejection so comes across as having a chip on his shoulder.
The extremely high-DEF score (above the 98th percentile) questions the Low Probability Result. As suggested, If the DEF is 8 or more, that increases the possibility of the SASSI missing individuals with a substance use disorder. It does not invalidate the result. There are many reasons for a high DEF – it could be situational – and it is not unusual in custody disputes to see a high DEF. It could be the client was defensive around their substance use. It could be that he has a defensive personality in general. The administrator is tasked with determining the meaning of the DEF scale score. It also tells you how to clinically approach a client who has difficulty opening up, is hypersensitive to others and is defensive.
The SAM score, though low, is the only scale which does not have an individual clinical interpretation. It is used in the decision rules to increase the validity and accuracy of the other scales it is paired with. It is also used to ascertain if the client is defensive around their substance use if both the DEF and SAM are elevated.
The FAM and COR results are not clinically significant.
In this kind of a case, the question of what timeframe to use with the FVA and FVOD scales comes up. It depends on several factors. Lifetime does give you an overall baseline of substance use but if you want a more “focused” timeframe, the last twelve months should be considered. Sometimes there is the issue of missing someone who had a significant issue in the past but is not currently using it, so a high probability result becomes a risk statement. A reminder: the SASSI cannot determine what a client is currently doing. This inventory is part of the information gathered by the administrator which is incorporated into the whole assessment.

