The SASSI Institute supports community corrections by providing tools, training, and resources to help probation officers, case managers, and other professionals identify substance use issues among individuals in the criminal justice system. Our tools can enhance decision-making, reduce recidivism, and support successful rehabilitation efforts.
Key Ways the SASSI Institute Supports Community Corrections:
1. Validated Screening Tools:
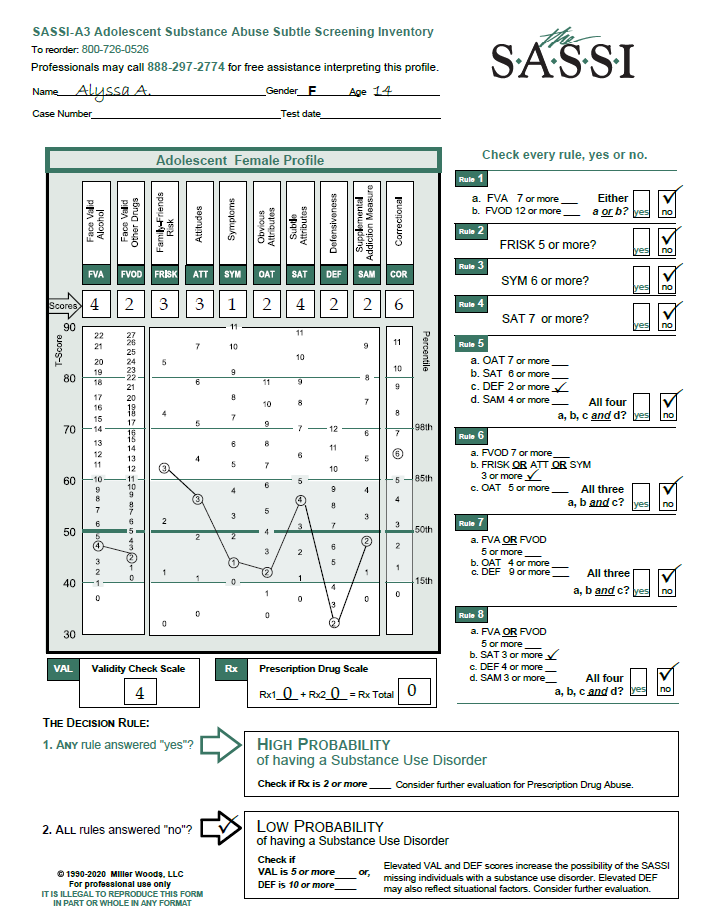
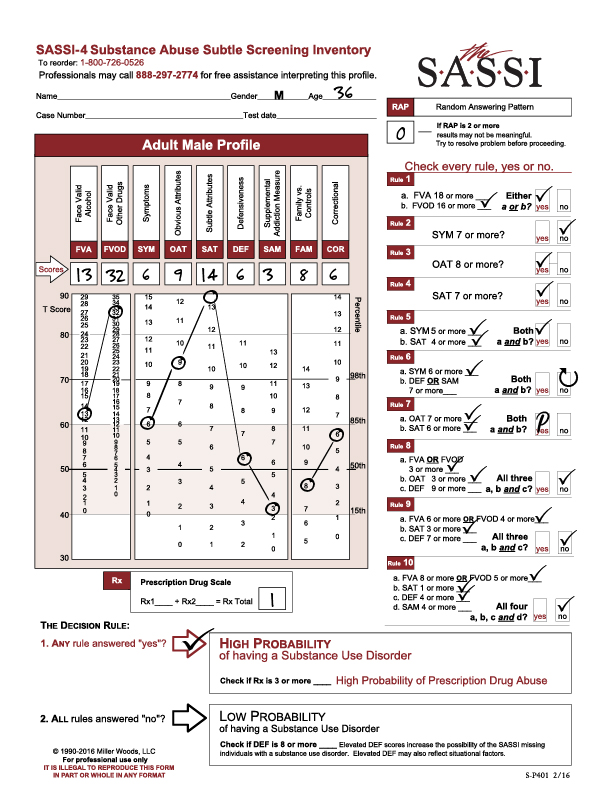
- The Adult SASSI-4 and Adolescent SASSI-A3 are effective tools for identifying substance use disorders, even in individuals who may deny or minimize their use.
- The Correctional (COR) scale may be useful in promoting discussion of the basis of clients’ legal difficulties, if any, and behavioral patterns that prompt other types of sanctions. Discussions focused on ways to avoid future problems can be valuable for the client.
2. Efficient Assessment Process:
- SASSI tools are quick and easy to administer, typically taking 15 minutes to complete, which minimizes disruption to case management workflows.
- Scoring can be completed manually or through online software, allowing for rapid scoring, interpretation and integration into case plans.
3. Objective Decision-Making:
- The SASSI provides objective scoring to support probation and parole decisions and help in identifying high-risk behaviors.
- Can help in determining appropriate levels of intervention based on the likelihood of substance use disorders and scale scores.
4. Treatment Matching and Referral:
- The SASSI can offer insights into individuals’ substance use patterns and behaviors, aiding in referrals to suitable treatment programs.
5. Training for Community Corrections Professionals:
- The SASSI Institute provides workshops to train professionals in using SASSI tools effectively.
- Training ensures probation officers and case managers can confidently interpret results and apply them in their work.
6. Reducing Recidivism:
- By identifying substance use issues early, SASSI tools help community corrections professionals intervene before substance use leads to further criminal behavior.
- The SASSI can supports rehabilitation efforts by addressing substance use as a contributing factor to criminal activity.
7. Resources for Special Populations:
- Offers tools and guidance for working with diverse populations, including adolescents, monolingual Spanish speakers and IAmerican Sign Language.
8. Ongoing Support:
- Access to our Free Clinical Help Line for assistance with interpreting results and addressing case-specific questions.
- Updates and resources to keep community corrections professionals informed about best practices in substance use screening and assessment.
Benefits of using the SASSI in Community Corrections:
- Enhances the ability to identify and address substance use issues in justice-involved individuals.
- Improves treatment outcomes and supports long-term rehabilitation.
- Efficient and reliable screening tools reduces workload.
- Strengthens the link between corrections, treatment providers, and community resources.
The SASSI Institute can help community corrections professionals make informed decisions, improve client outcomes, and contribute to public safety. Large volume SASSI users in federal, state, and local correctional centers can reach out to us about the development of customized reports on a contractual basis to meet specific program needs