Although there have been ample demonstrations of the value of rehabilitation programs for criminal offenders, it is important to recognize that recidivism in the criminal justice system remains a serious problem.
It would be an easy matter to greatly reduce the incarcerated population if one and only one factor caused people to have multiple arrests. Substance Use Disorder (SUD) is a strong common element among repeat offenders. However, there are numerous other factors that can also lead to habitual legal offensives – impulse control problems, personality disorders, psychiatric disorders, cognitive impairment, chronic stress, a history of trauma, childhood and other developmental issues, peer culture, poor social skills, etc.
No single factor necessarily causes criminality, but each one can contribute to a tendency toward law violation, and they can combine to produce a high-risk profile. Because there are multiple causes of criminality, one treatment program may be of value for some repeat offenders but still does not address all the issues that need to be addressed to prevent further legal difficulties. Repeat offenders do not come from one mold. Therefore, one given course of treatment is not likely to be maximally effective for all recidivists.
Screening to Identify Risk
The challenge of early intervention is to find a means of identifying and addressing risk. A first step in reducing recidivism in the criminal justice system is to screen legal offenders to identify individuals who are at greatest risk for ongoing legal difficulties and who are likely to have an SUD to provide them with appropriate and timely treatment.
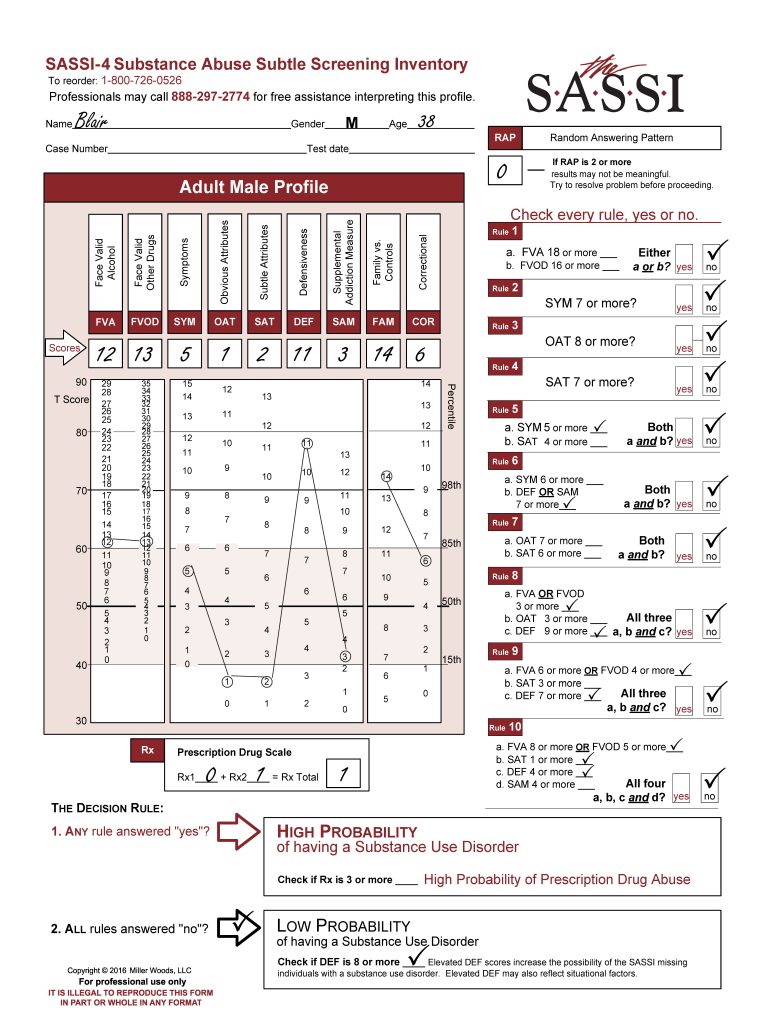
SUD is strongly related to legal problems. Using SASSI screening tools can provide information on ongoing legal problems that can be helpful in treatment planning. Since there are multiple causes of habitual offending, instruments that measure a single factor are not likely to be effective in early identification of high-risk individuals. The SASSI Correctional (COR) Scale identifies individuals with a history of legal problems. While it is unclear why the COR items identify these individuals, there are many possible factors to explore, including: impulse control, anger management, high risk-taking, not responsive to consequences of behavior, low frustration tolerance, and poor social skills.
Effective Screening
Screening is a first step; but a vital and cost-effective first step, particularly in settings that process large numbers of clients. After identifying high-risk individuals, it is important to gather information that is useful in developing a treatment plan.
Client-Appropriate Treatment
There is real value in gathering information that is directly useful in planning therapeutic interventions that will address the client’s specific needs. When screening and assessment are conducted with the intent to help the professional join the client in setting effective treatment goals and planning how to achieve them, the screening and assessment becomes a vital part of the treatment process. It is important to use tools that are accurate and provide clinically useful information.
Despite the overall effectiveness of SUD treatment and despite the demonstrated cost-effectiveness or providing treatment as part of society’s response to criminality, rehabilitative diversionary programs are not maximally effective in reducing rates or recidivism. Part of the solution lies in developing interventions that are sensitive to subgroup differences and individuals’ needs. Individuals with SUD differ from one another. They therefore respond differently to different types of treatment.
Matching treatment on the basis or the nature and degree of the client’s psychopathology and sociopathy increases the effectiveness of the treatment. While it may not be possible to fulfill all the mandates, if we wish to reduce recidivism within the criminal justice system, it is necessary to identify the individuals most at risk, determine their treatment needs, and provide treatment tailored to those needs. The SASSI screening tools can be a very helpful first step in that direction.