Through the years, we have had the opportunity to share inspirational stories with our colleagues about their experience using the SASSI. One such story came recently from a psychologist who uses the SASSI in his practice. This was a gratifying story for us to hear and we are pleased that he has allowed us to share it with you.
The mother of a 22-year-old woman called me because she felt very strongly that her daughter Aimee (not client’s actual name) had an alcohol problem. But Aimee was adamant, no question about it, “I don’t have a problem.”
After some persuasion, Aimee agreed to come into my office, and I invited her mother to stay in the office during the interview, with Aimee’s permission. I really think Aimee was very certain that there wasn’t a problem, and that having Mom there during the process would convince her mother of this, too. I said, “You know, Mom can be a bit of a reality check here, but I’m listening to what YOU are saying.” Aimee’s mother agreed to just listen, since she had had her say when making the referral.
We talked about it, and Aimee restated that she didn’t have a problem. She was just not aware of any bad consequences coming from drinking. Aimee really seemed to believe what she was saying, “My friends and I, we don’t have any consequences; we just enjoy drinking.” I told her that was fine and asked, “Would you like to find out if you, in fact, do have a problem, or would you rather not know?” Of course, this is right in front of Mom. And she thought about it, seeing herself as being free to say “no.” But she did say, “Yeah, I think I would want to know.” When asked about each of the DSM diagnostic criteria for substance use disorders, Aimee answered no to all symptom questions.
Then, I brought out the SASSI-4, and told her a little bit about how it would compare her responses to two known groups of people: those who have a problem and know it, own it, and the other group that is just as aware that they do not have a problem, and own that. And we will see how your responses go. She agreed that that sounded good. She took the SASSI-4, and her responses showed a high probability of having a substance use disorder. This was very surprising to her. Then I went back and showed Aimee her scores on the FVA and the SYM.
When she looked at those scores, she could see by the profile that the consequences she was getting were way out of line compared to ordinary people who drink. She runs with folks whose norm is to drink a lot, and there is a history in her family of substance use issues. She just said, “It’s almost like thinking about it and realizing that you are surrounded, and your best bet is to give up!” She surrendered to the idea that, “Yes, I’ve got a problem.” From there on she was willing to do something about it. Aimee made an appointment to see me again, and we went on from there.
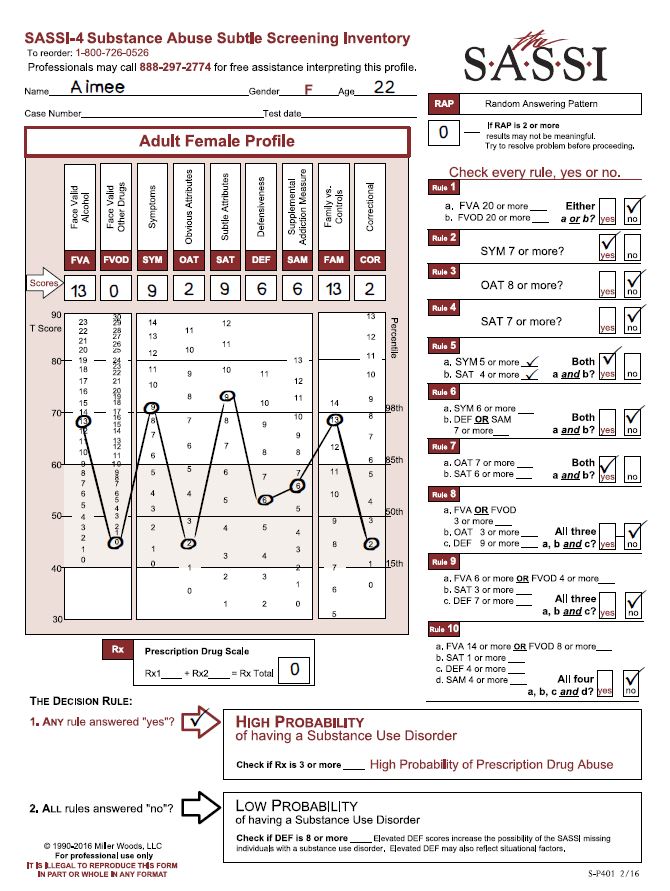
Let’s say that the SASSI did not exist, and I would have had only the DSM criteria and her history. I would have had her mother’s reflections and thoughts and observations, and—I don’t feel certain, but I’m guessing—she would have walked away with the understanding that she did not have a problem. She would have gone on as she had been—because I would not have been able to make a case that she did have a problem, because there would have been no data to base that on. She may well have been one of those who left the interview, and for the rest of her life said, “No, I don’t have a problem, so get off my back.” In a sense, I really believe that the SASSI saved this young woman’s life, or at least spared her significant pain. I have always been impressed by the accuracy of the SASSI. It picks up on people who really are “sincerely deluded.” It’s interesting that her score on the Defensiveness (DEF) scale was not particularly elevated, so it was not that she was being defensive, she was just unaware of how her drinking and symptoms associated with it were beyond the norm. Her elevated SAT score – at the 98th percentile – supports the interpretation that Aimee has little insight into what may be motivating her to drink with her friends, or the negative consequences that follow from spending time that way. I am very grateful for the SASSI, and I wouldn’t do an assessment or a screening without it. I literally would refuse, because just the verbal reports can be so misleading, although not intentionally misleading, necessarily. Clients will compare themselves with the people they know who are much further along in the addiction process, and not really understand that their own behavior is a problem, just because their own behavior is not yet as severe as what they see in others. The SASSI can put a client’s use into a broader, and often more realistic context.
Original depiction, written by Nancy Winningham, M.A. based on an actual experience a clinician had using the SASSI with a client. Adapted to reflect SASSI-4 information.