Engaging in assessment regularly can make it become routine; therefore, sometimes perspective is lost and the purpose forgotten. Time needs to be taken to remember the precise questions assessments are trying to answer. When forgetting the specific reasons for conducting assessments, they lose their value both to the individual client and the clinician.
Screening is an important part of assessment for the purpose of triage, identification of risk factors, and referral for additional services. The basic question is whether an individual is likely to have a particular problem. If so, the subsequent assessment and treatment plan should address that problem. Since screening tools are used to identify people who are likely to have a problem or be at risk for developing a problem, they are never infallible. The key element is to use a screening tool that meets the needs of the clinician. As an example, the crucial factor in airport security screening is that the procedure be highly sensitive; they do not want to miss anyone who is a security risk. ln other words, they do not want any false negatives. However, in eliminating all false negatives, the procedure that is used produces false positives and anyone carrying metal is flagged by the airport security screening and given some degree of further scrutiny, even though most people who carry metal are not found to be a security risk. But different screening settings have different needs. ln developing and maintaining the SASSI, the researchers recognized that there are costs associated with both over and under-identification of substance use disorders (SUD). Therefore, the research and development aims were directed toward maintaining a high level of sensitivity (few false negatives) and a high level of selectivity (few false positives).
While a relatively comprehensive assessment may be needed to arrive at a diagnosis, the basic question is whether the individual meets the specific criteria (e.g., DSM-5) necessary to arrive at a diagnosis. There exists a long-standing controversy regarding the value of diagnoses. Some argue that diagnoses serve to label people unnecessarily and others argue that it is important to do whatever possible to specify an individual’s problem in a reliable and meaningful manner to ensure appropriate treatment recommendations. Regardless, most agencies require clinicians to formulate a diagnosis, and diagnoses are needed for third party payments and as part of the admission criteria for many treatment programs.
Assessments are also needed for reports. Often individuals are referred by outside agencies (e.g., other health service providers, courts, employers, schools). In these instances, the clinician is placed in the position of providing expert opinion in what may be controversial or even litigious situations. It’s vital for the clinician to have a clear understanding of the precise request being made by the referral agency – What are the questions to be answered? What are the issues that are to be addressed? What types of opinions and recommendations are requested?
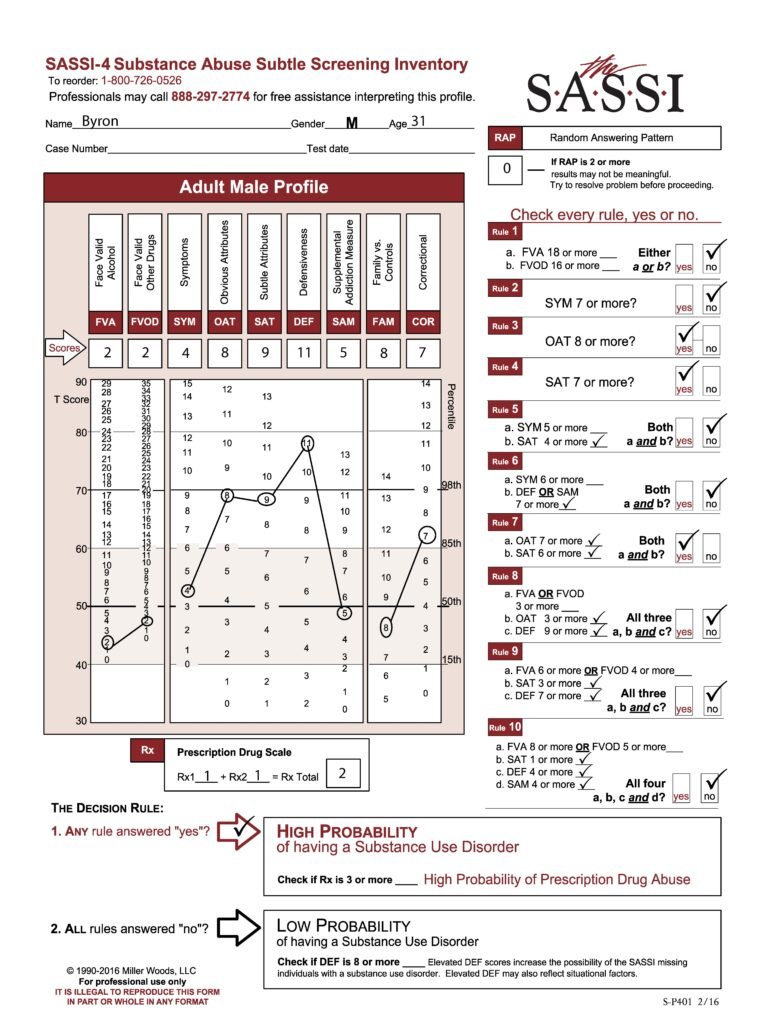
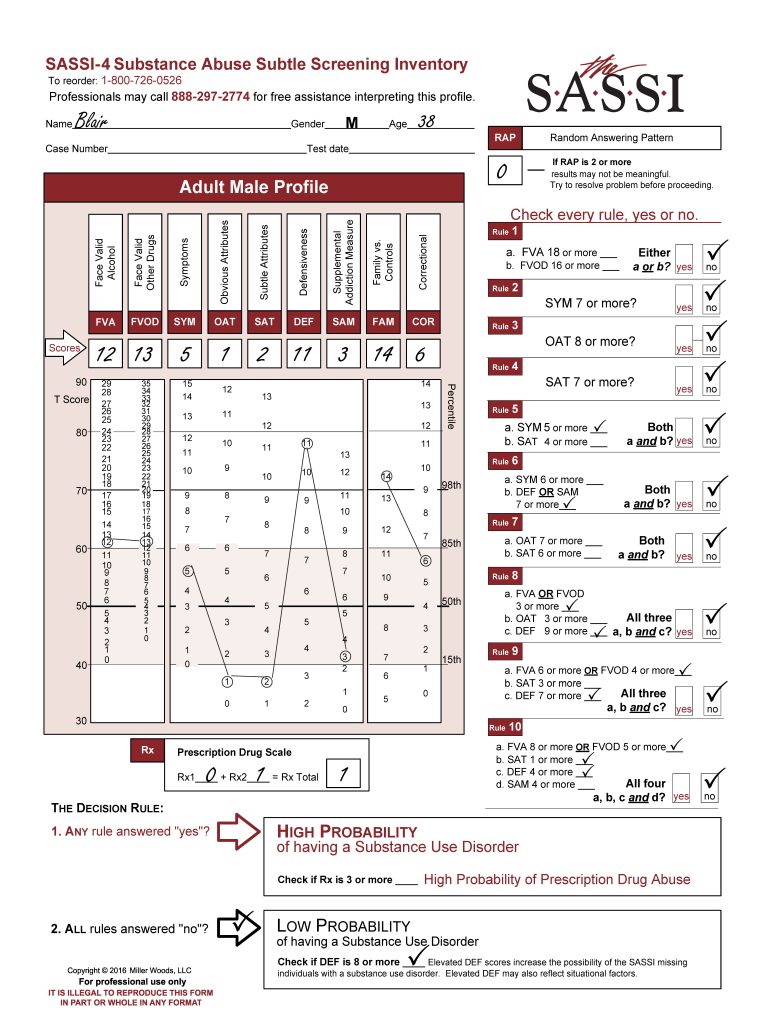
In conducting the assessment and writing the report, the clinician should be clear in differentiating observations from inferences and opinions. For example, if the only information on frequency and quantity of consumption of alcohol and other drugs is the individual’s self-report, the written report should indicate that the individual reports using a certain amount, not that the individual actually consumes that amount. If the clinician has cause for concern regarding a symptom of SUD, it should be phrased as a cause for concern rather than an observation. When using the SASSI to screen it becomes possible to make a statement to the effect that the individual’s pattern of responses suggests, with a known level of certainty, that the client is or is not likely to have an SUD. (Note: In addition to screening results, supplemental clinical information is required to meet the accepted standards for a DSM-5 clinical diagnosis of an SUD). The SASSI Rx scale can also help identify individuals likely to be abusing prescription medications and the other additional scales can provide clinical insight into level of defensiveness, consequences of use, desire for change, family and social risk factors, and acknowledgement of problems.
Always present information clearly and distinguish observation from inference and opinion. It is important to help the individual become increasingly invested in the treatment process. Assessment is a critical part of the treatment process and provides an opportunity for the clinician and the individual client to mutually identify problems, set goals, and devise strategies to meet those goals. The individual client is the primary focus, and the information that’s gathered is useful to these individuals only to the extent that it helps them take action that enhances their quality of life. For information on interpreting SASSI scales, please consider completing our Clinical Interpretation training. Registration information can be found at https://sassi.com/sassi-training/. Also, professionals can call our free clinical helpline at 800.726.0526 Option 2, M-F 1-5pm ET for help with profile interpretation.