This is an interesting profile on a 23-year-old male as it brought up the question, we get on the helpline regarding video gaming. “Does the SASSI evaluate for video gaming addiction?”, especially if the administrator believes the client was possibly including video gaming as well as substance use in his answers. The simple answer is no, it does not, so please clarify with your client not to include video gaming. A drug that is often associated with video gaming is Adderall so the follow-up question to a client who admits to excessive video gaming is to question what drugs are they using to maintain that level of energy and concentration.
This individual was instructed to complete the FVA/FVOD side of the questionnaire for the last 12 months.
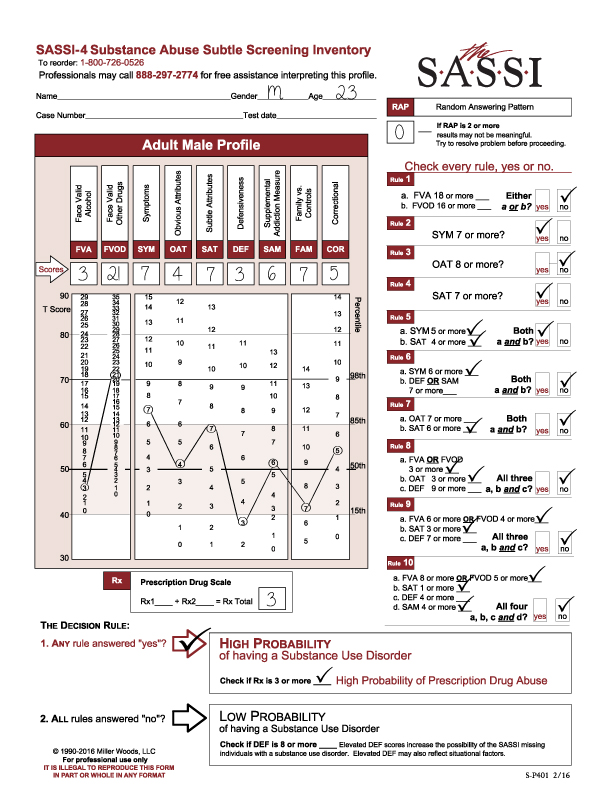
RAP was 0.
High Probability of a Substance Use Disorder.
Prescription Drug Scale result was 3 so meets the cutoff for High Probability of Prescription Drug Abuse.
He met Rule 1 with a FVOD score of 21.
Rule 2 with a SYM score of 7.
Rule 4 with a SYM score of 5 (7) or more and a SAT score of 4 (7) or more.
Looking at the graph on the Profile sheet, you will see a significant elevation on the FVOD scale score – above the 98th% so he is openly acknowledging use of drugs. By analyzing his responses, you will gain insight into what circumstances he is using, including dealing with emotional or stressful issues. And remember, he is answering the FVOD questions based on the last 12 months.
The SYM elevation is above the 85th percentile – enough to meet Rule 2. Because SYM is a face valid scale, you can do content analysis on those questions to look at the symptoms and consequences of his substance use.
The OAT score is within the norm. It would probably be the case that he does not identify with other substance abusers. This may be related to his very low-DEF score.
The SAT score is within the norm but high. The administrator may pick up some denial or lack of insight on the part of the client. And again, it may be related to the DEF score.
The DEF score is very significant because it is so low, below the 15th percentile. This individual may be in emotional distress and may be suffering from depressive symptoms. He should be evaluated for depression as he may be using substances to self-medicate. He may also believe that if he wasn’t depressed, he would not be abusing substances thus the OAT and SAT scores may reflect this perception.
The Rx score is also very significant and warrants further investigation as to what prescription drugs he may be abusing and if, in fact, are related to video gaming.
The rest of the scores are within the norm, so not clinically significant.
In summary, these clinical results are hypotheses to explore with the client to determine the depth and scope of the client’s use in order to recommend a treatment plan which fits his particular needs.
We hope this is helpful to you.
The clinical helpline line is open for your inquiries, M-F, 12- 5 (EST) at 888-297-2774 and you will be directed to a clinical consultant. If we are not available, please leave a message and we will return your call.
And as always, Thank you for your interest in the SASSI.
PDF Version Available for Download