
The SASSI Institute is proud to share one of our newest manuscript addressing adolescent substance abuse. The title of this article is Mandated Treatment for Troubled Adolescents and Substance Use Disorder: Identifying and Breaking Through Defensiveness and Denial. It provides an investigation of the defensiveness demonstrated by teens who are mandated to participate in treatment as compared to their non-mandated peers. Part of the data set we collected for The Substance Abuse Subtle Screening Inventory (SASSI) Institute’s third iteration of the Adolescent SASSI-A3, the present study focused on data from 164 mandated teens that participated in the principal study. As in the principal study, these cases were drawn from substance use treatment, criminal justice programs, community corrections, and private clinical practices, among other venues, and all cases were provided by clinicians working within these service settings throughout all U.S. Census Regions. In addition, we review cases demonstrating high-levels of defensiveness and denial in these mandated teen clients, and ethical ways to break through that barrier towards effective treatment engagement. Finally, we present two brief de-identified treatment case studies, aptly demonstrating defensiveness and denial from a clinical standpoint. We at The SASSI Institute are very proud of this work, and I want to personally thank my co-authors for making this work possible. The article is available free of charge as it was submitted as an open-access article distributed under Creative Commons Attribution 4.0 International License (CC BY 4.0), which allows readers to copy, redistribute, remix, transform, and reproduce in any medium or format, as long as the original authors are properly cited.
Tag: Substance Use Disorder
Psychopharmacology and the Biology of Addiction Webinar
Increase your understanding of how drugs of abuse interact with each other as well as what takes place in the brains of experimenters, abusers and addicts. Improve your ability to communicate with medical professionals and your clients.
On March 29th and 31st, 2022, Dr. Donald R. Osborne, Jr., author of the newly released book “You Can’t Fall Out of a Hole: Ripping the Band Aid off of Our Addiction Epidemic,” will be hosting a live webinar to increase your knowledge on the subject of Psychopharmacology and the Biology of Addiction.
Information that will be presented and discussion will be about the following:
| Central Nervous System | Peripheral Nervous System |
| Autonomic Nervous System | Somatic Nervous System |
| Sympathetic Nervous System | Parasympathetic Nervous System |
| How the Brain Works | Tolerance and Cross-Tolerance |
| Rebound / Withdrawal | Drug Half Life / five to eliminate |
| THIQ in Alcohol Metabolism | Dopamine Depletion by Cocaine |
| Determining BAC by number of drinks consumed |
The following drugs/drug classes will be examined:
| Opioids | Alcohol |
| Sedative-Hypnotics | Cannabis Sativa |
| Cocaine | Sympathomimetics |
| Inhalants | Hallucinogens |
| Club Drugs | Caffeine |
| Nicotine |
For each of the drugs/drug classes, the following information will be provided and discussed
- Examples
- Route of Administration
- Absorption
- Distribution
- Effects
- Metabolic Half-Life
- Elimination
- Rebound/Withdrawal
The webinar will be live from on March 29th, 9:30-1pm ET, and March 31st, 1:30-5pm ET. The webinar will be available on-demand afterwards.
To register, click the date you are interested in below:
Reviewing an Adolescent SASSI-A3: Vaping Issue
This is an issue that may be turning up in your clinical practice. The caller wanted help with a profile interpretation on a 13-year-old male who had turned in a vaping pen. The school was mandated to do a substance use evaluation as a result. The online report indicated “inconsistencies” in the results so the counselor wanted more information. The client was instructed to complete the FVA/FVOD side for his whole lifetime.
The overall result, based on all the rules being ‘no’, came up with a Low Probability of a substance use disorder. The Prescription Drug Scale was zero. However, the Validity Check Scale was 6 so further evaluation was recommended. Elevated VAL and DEF scores coupled with a Low Probability result increases the possibility of the SASSI missing individuals with a substance use disorder.
Looking at the graph on the profile sheet helps to pull out additional information. Note the very low (below the 15th percentile) OAT and SAT scores. The low OAT can indicate someone who has a hard time acknowledging personal limitations or shortcomings. The low SAT can indicate someone who has a chip on their shoulder, feelings of rejection and hypersensitivity to others. Interestingly, the DEF score is within the norm and does not indicate the student was defensive completing the SASSI. The FRISK score is above average but within the norm and because it is a Face-valid scale, content analysis of those items may be useful. The other Face-valid scales, ATT and SYM with their scores of 1 can also be examined.
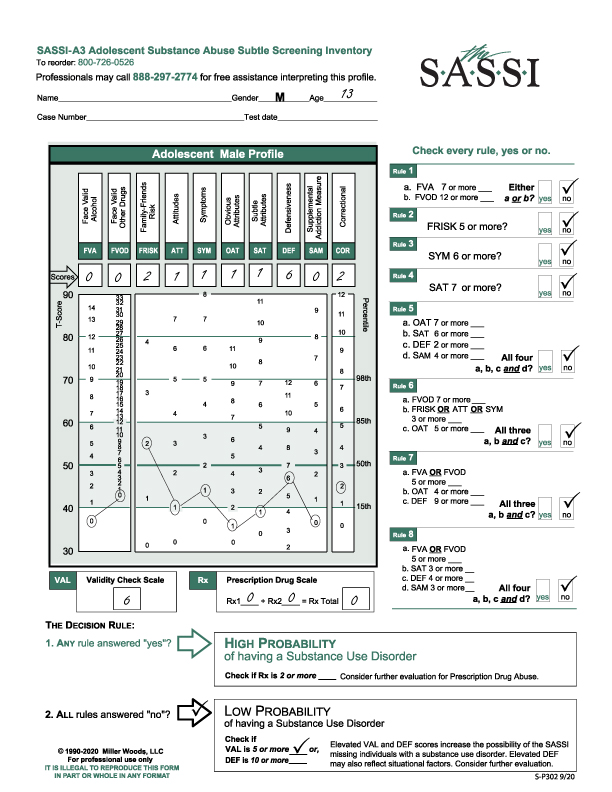
The student who turned in the vaping pen indicated it was not his. It was not clear from the caller what substances they suspected were being used. Clinically, the best thing to keep in mind is that the student has a hard time opening up and is probably very concerned about how he is viewed by teachers, counselors, etc. and very quick to feel rejected. Interacting with him in an accepting and affirming way is probably the best approach.
Substance use issues: The VAL of 6 is a red flag so further evaluation with this student is warranted. It could be on-going oversight within the school, i.e. school counselor or referral to a Substance Use counselor who could do a more formal and comprehensive assessment.
We hope this is useful for you.
As usual, don’t hesitate to call the Clinical Helpline at 800-726-0626 with any clinical questions. Live clinicians are available M-F, 11-5 pm (EST). Otherwise, feel free to leave a message and we will get back to you the next business day.
Profile Configurations: When the OAT is higher than the SAT vs when the SAT is higher than the OAT
One question we field often on the clinical helpline is what does it mean when either the OAT (Obvious Attributes) is higher than the SAT (Subtle Attributes) or when the SAT is higher than the OAT when both are elevated above the 85th percentile?
New Workshop: Community Reinforcement Approach for Substance Use in Adults
We hope some of you have been able to participate in at least one of our new Professional Development webinars. We are excited to be able to partner with fellow colleagues in the field of addiction to be able to provide continuing education on professional topics of interest.
We have recently partnered with Courtney Hupp, MSW, LCSW, CADC, an EBT Clinical Coordinator at Chestnut Health Systems in Illinois. She had an active role in the Assertive Continuing Care (ACC) study, funded by NIAAA, in which she administered the ACC and Community Reinforcement Approach (CRA) protocols to residential clients’ post-discharge, as well as supervised other therapists on the study. Courtney will be offering her workshop “Community Reinforcement Approach for Substance Use in Adults” live online through the SASSI Institute’s training platform on February 8th. The treatment model known as CRA recognizes that, at least initially, alcohol and drug use is about reinforcing consequences — that make us more likely to repeat actions. This is true whether we are hanging out with friends, playing a favorite game, eating a good meal, or using alcohol or other drugs. People who use alcohol and drugs get something out of it – or they wouldn’t keep doing it.
The overall goal of CRA is to help individuals reconnect with or discover new sources of positive reinforcement within their community to compete with alcohol or drug use. How do CRA clinicians do this? By listening to and learning from their clients what is important to them. They then help them connect to pro-recovery activities that have meaning and value to their client. In addition, CRA clinicians help their clients identify goals and learn how to achieve them. CRA clients also learn a variety of new skills, such as problem-solving and positive communication (with partners, friends, and others), which help them attain a better quality of life. Practicing new skills is a critical component of the skills training used in CRA. Every session ends with a mutually-agreed upon homework assignment to practice skills learned during sessions. This intervention has been implemented in outpatient, intensive outpatient, and residential treatment settings. This research-tested intervention has been used in over 500 organizations across the United States and Canada. Courtney Hupp will provide an introduction to the CRA model, a summary of the research base, and details about how to use a variety of CRA skills during sessions.
What You Will Learn:
- An Introduction to the CRA model
- History of CRA research and implementation
- Goals of CRA treatment
- An overview of the CRA session structure and treatment guidelines
- How to use some of the CRA procedures during sessions like a Functional Analysis for substance use, Happiness Scale, Sobriety Sampling, and Increasing Prosocial Recreation
- General clinical skills necessary to implement CRA
For registration information click here.
A SASSI-4 Profile Analysis: Prescription Drug Abuse
A caller requested help interpreting the result of a SASSI-4 questionnaire on a male client who presented himself as having an opioid addiction.
‘Curtis’ is a 36-year-old married man. He and his wife have no children. He works as a landscaper which he describes as physically very demanding. His parents smoked marijuana while he was growing up and Curtis also smokes marijuana. His older brother died ten years ago, and Curtis is still grieving. His brother also had substance use issues. Curtis also may have a history of being molested as a child which he does not remember, but his brother relayed that they were both molested by a babysitter.
Curtis reports a four-year history of opioid addiction which started as a result of a herniated disc in his back. He was initially prescribed hydrocodone for pain. He tried to quit once three years ago. Currently, he is ordering “stuff off the internet” or getting oxycontin from friends. He has been taking 180 mg/day with a maximum of 240 mg per day. It takes 150 mg. for him not to get “sick.” Curtis continues to smoke marijuana on the weekends about one time per week. He has a legal history of possession of marijuana in 2004 and attended an outpatient treatment program doing “what I had to do.”
He has been slowly tapering off the opioids for the past five weeks and currently is down to 80 mg/day. His goal is to completely get off the opioids but he is not interested in residential treatment at this time because it is his busiest time of year. Although he has attended NA, he does not like it. Curtis is more drawn to Smart Recovery.
The SASSI-4 was administered for lifetime use on the face valid side of the questionnaire.
What were his SASSI-4 results? Curtis has a ‘High Probability of having a Substance Use Disorder’ and a ‘High Probability of Prescription Drug Abuse.’
This looks like a straightforward profile on the face of it. His score of 42 on the FVOD and 18 on the SYM indicate someone who is very open concerning his drug use, and because these are face valid scales, content analysis could provide useful information to further explore with the client.
The OAT score of 6 is right at the 85th percentile. The client may be able to identify with some of the characteristics of substance users such as impatience, resentment, self-pity and impulsiveness. However, the SAT score of 8 is higher than the OAT and may blunt the ability for Curtis to have insight into his behavior. When the SAT is higher than the OAT, the client may exhibit a lack of awareness or simply denial around the impact drugs are having on his life. In this case and not unusual, opioid users do not see themselves as “typical” addicts. That may account for the OAT score.
The DEF score of 2 can be a ‘red-flag’ as it is below the 15th percentile. A score this low can indicate someone with poor ego strength, feeling helpless and hopeless and may be exhibiting symptoms that look like depression. The clinician may want to do a mental health screening or refer the client for screening.
The FAM score of 5 is also very low, below the 15th percentile. This can indicate the client is focused on himself and not that concerned about others. This does not indicate a personality disorder but given the client’s circumstances, makes sense that he would be more internally focused.
The COR score of 8 is elevated above the 85th percentile. He has answered in a similar way to people who have had legal issues for any reason. We suggest screening for those behaviors or characteristics we often see in that population. These can range from poor social skills, low frustration tolerance, risk-taking behaviors, anger management issues or impulse control issues. These issues could be impacting on Curtis’s choice-making abilities.
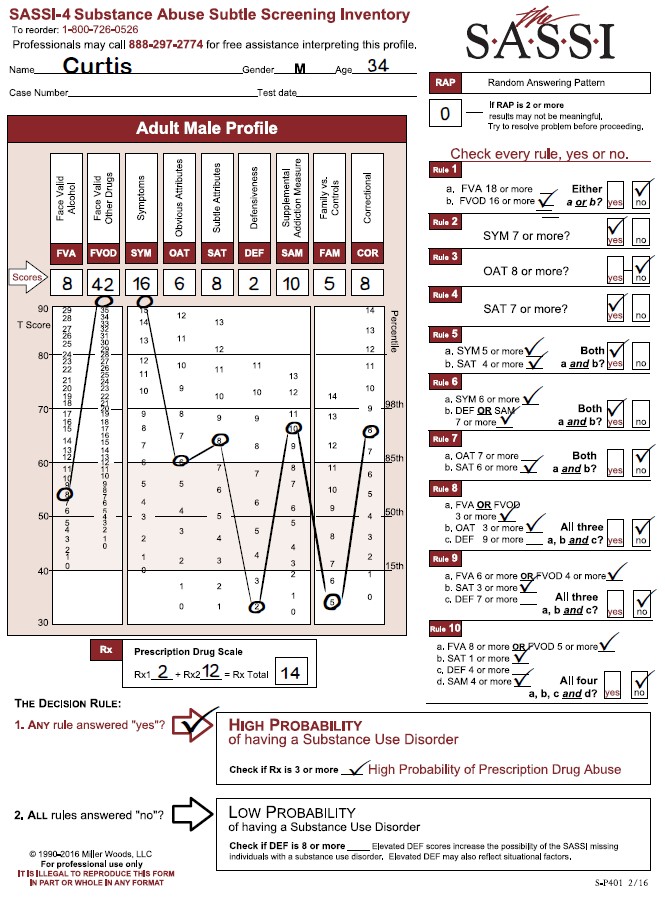
Finally, looking at the Prescription Drug Scale. With the score of 14, it is quite clear that he is identifying behaviors associated with prescription drug abuse. Again, as a face valid scale, looking at these individual items will generate a lot of information for the clinician. The clinician will need to look at treatment readiness, discuss medication needs, possible referral and other reported clinical issues.
A SASSI-4 Profile Analysis: Context Matters
If you have attended one of our trainings either in-person or online, you know the section on how to administer the SASSI to a client is one of the most important. A thoughtful approach can set the tone for the entire assessment by helping a client feel more at ease and engaged in the treatment process. We emphasize the importance of first establishing rapport with the client. The questionnaire is presented as an aid, not a test with right or wrong answers. We instruct to administer the true/false side first, then checking the appropriate time frame for the face valid side. Letting the client know s/he will have a chance to discuss the results at a later time increases the client’s comfort level.
Our protocol is based on the recommended one-on-one consultation. We realize that is not always possible. Administrators of the SASSI work in a variety of settings including schools, probation departments, EAP, treatment agencies, institutions and private practice. Since the SASSI does not require a professional to administer it, a variety of personnel can be trained, but both the context and the administrator can have a significant impact on the receptivity of the client.
This example of the context of a SASSI given to a client dramatically shows the difference the setting can make in the results. One of our clinicians fielded this call. The administrator did not know which results to use even though both profiles came up with a high probability of having a Substance Use Disorder.
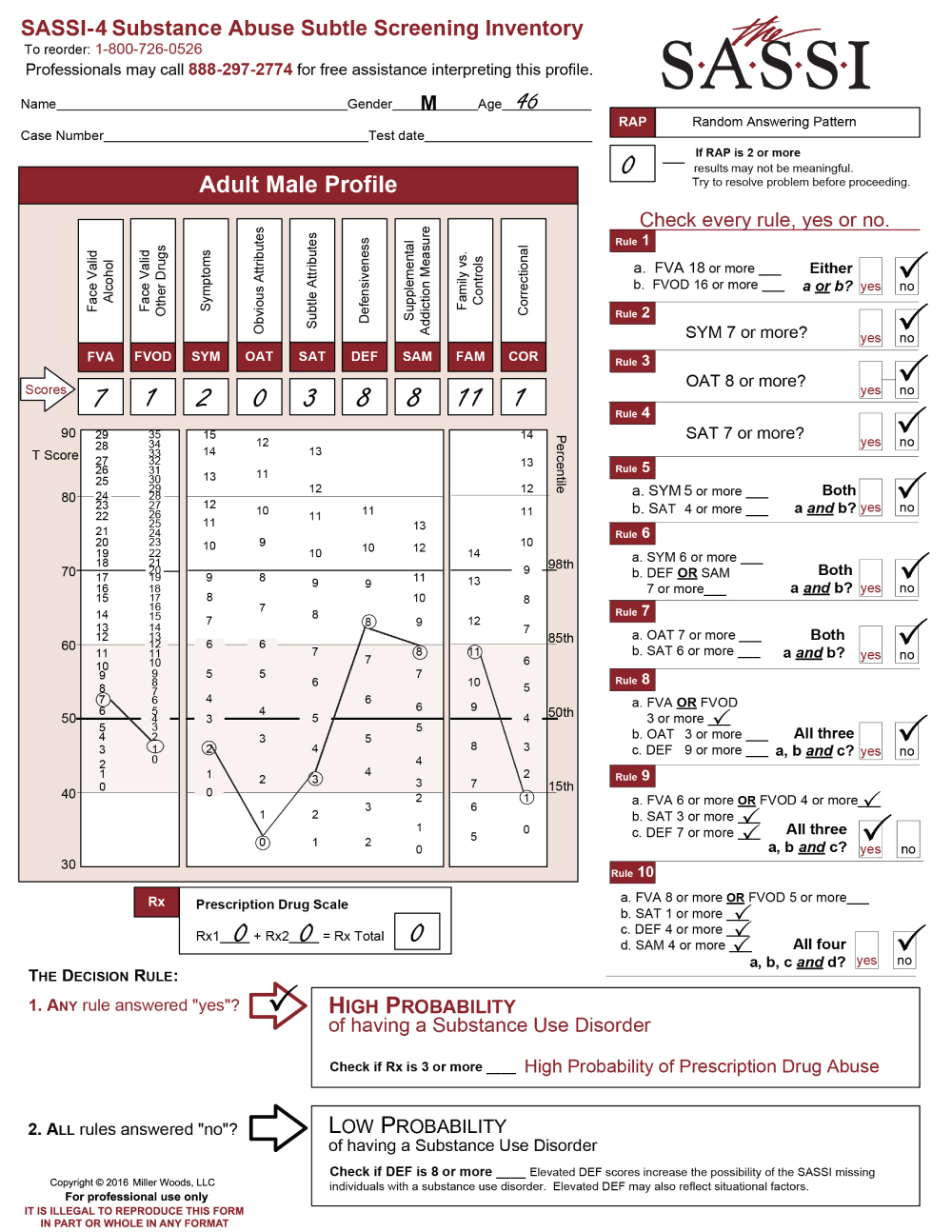
The client is a 46-year-old male who was given the SASSI at the Courthouse in a packet of material he was instructed to complete. Two weeks later he was given another SASSI to complete. This time with a counselor assigned to evaluate him.
Here are the results of the first SASSI he completed at the Courthouse:
As you can see, he meets Decision Rule # 9. Looking at the graph, some scales and numbers stand out. On his face valid scales, including SYM, his numbers were within the norm, between the 15th and 85th percentile. His OAT score is extremely low which indicates he has a hard time acknowledging personal limitations or shortcomings and may have difficulty in groups. The other significant score is the DEF score of 8. In spite of the elevated DEF score, he did meet one rule. The SAM is almost at the 85th percentile so, in my mind, I might be more inclined to say he was defensive about his substance use and perhaps minimizing on the face valid scales. This hypothesis would depend on the rest of the assessment with any additional information. However, he was given the SASSI to complete within a packet of materials, and it is very unclear what instructions he was given, if any, on how to complete the SASSI.
Let’s look at the results of the 2nd administration given just two weeks later in the office of the counselor who was evaluating him after meeting and talking with the counselor.

In this profile, the client meets multiple decision rules including numbers 3, 4, 5, 6, 7 and 10. All it takes is one rule to meet high probability and more than one does not mean a more severe substance use disorder. Diagnosis and severity are based on the DSM-5 criteria. It is evident his raw scores have changed to impact the decision rule results.
There is a significant change in his Face Valid Scales with an FVA of 11 and an FVOD of 14. His SYM score of 6 also shows elevation. OAT has changed from a 0 to a 9. He is now indicating a willingness to acknowledge shortcomings and limitations. In addition, he probably can identify with other substance abusers so a referral to a group treatment program can be considered.
The significant drop in the DEF score from an 8 to a 5 is nice to see. The client met with the counselor who was able to establish rapport by making the client more comfortable and explaining what the SASSI is and how it will be used in the context of the assessment. The low FAM score reflects the client’s internal state of mind. He is probably very concerned about what is going on within himself and not so concerned about others.
The final interesting scale change is the COR score and probably more representative of the client’s self- assessment at this point. Perhaps he is more able to identify impulsive or anger management issues, risk-taking behaviors, low frustration issues, or poor social skills. It gives the counselor some insight on what to explore, regarding behaviors which are impacting the client’s choices.
The most important difference in these two profiles was how the SASSI was presented to the client. Context, and establishing rapport can produce a more useful SASSI by obtaining a depth of clinical information. As an aside, we were not informed on why the SASSI was administered twice within a two-week time frame. We do not usually recommend doing so. It may have been the counselor was unaware of the first SASSI administration until receiving the completed materials from probation.
We hope you find this useful information regarding clinical issues. As always, the Clinical Helpline at 888-297-2774 is open to serve you Monday through Friday, 9 am to 5 pm (EST).
SASSI Identifies Rx Abuse (with video)
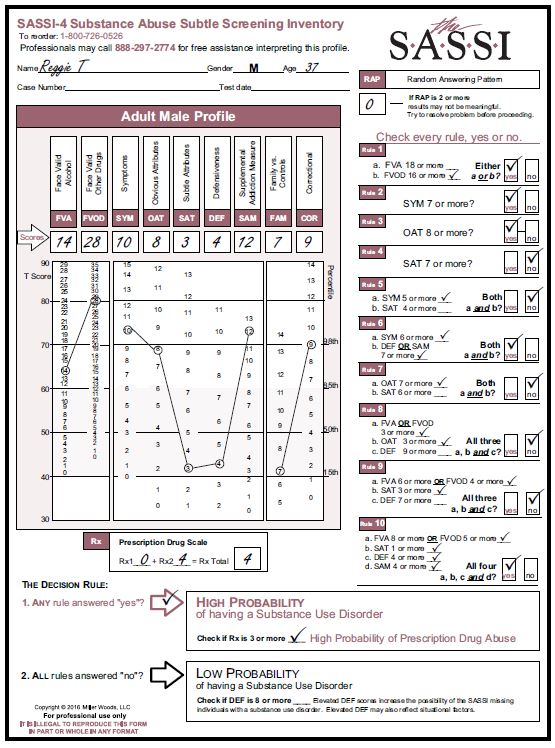
‘Reggie’ is a 37-year-old married man. He and his wife have two children. He works as a warehouse worker where he was recently injured in a shipping dock accident. He recently returned to work after being on worker’s comp for several months during which time he was prescribed opioids for his pain. He was sent to his employer’s EAP provider for evaluation after returning to work and struggling with coping with the continued pain and poor job performance.
Reggie T’s responses illustrate another profile often seen in people who acknowledge that they use drugs excessively and that it negatively impacts on their functioning and relationships.
Given Reggie’s high level of drug use and consequences, you might consider a more comprehensive evaluation to determine whether he may need supervised detoxification or other intensive intervention.
You may find Reggie ready to acknowledge that he uses drugs frequently and that he may also drink too much. However, he may not see that his behavior varies dramatically from others who don’t have a substance use disorder. Feedback on where his scores fall on the profile sheet may help him see that his behaviors are not typical. It may be useful to know that Reggie’s wife is currently in treatment for drug and alcohol abuse due to a DUI. Their mutual abuse of substances may help promote their beliefs that their substance use is normal. Examining the items that Reggie endorsed on the FVA, FVOD, SYM and Rx scales may provide useful insight into his motivations for using and help him see the consequences that result from his use.
In this first video watch Reggie’s initial EAP visit in which he was asked to take the SASSI.
This second video is the follow-up session where he discusses his SASSI results with the EAP provider.
A SASSI-4 Profile Analysis: Reading Aloud the Questionnaire and Interpretation of Low Scores
We regularly get inquiries about the acceptability of reading the questionnaire to a client who may have difficulty with their reading skills. We discourage the evaluator from reading the questionnaire to the client for a variety of reasons, but the primary one concerns the validity of the results. No matter how careful the reader might be, the tone of voice or emphasis on a particular part of the question may lead the client in one direction or another. Or the client may interrupt with a question regarding the meaning of a word or intention of a particular question. This is why we offer a professionally read audio CD of the SASSI-4, Adolescent SASSI-A3 and Spanish SASSI paper and pencil versions for clients who have reading difficulties. We hope in the future to be able to offer this for the online platform as well. Please contact our customer service department for ordering information.
Another frequent question is related to the clinical interpretations of the “low” scores on the profiles. These mostly relate to the subtle scales which include the OAT, SAT, DEF and SAM scales. Most callers know what a low DEF indicates. And SAM has no clinical interpretation.
So what about those low OAT and SAT scales? What does “low’ mean? A low score is anything below the 15th percentile on the graph. In the example to the right, the caller indicated that she was doing an assessment on a health care professional who had been arrested for her one and only DWI the previous year, had completed her alcohol education class and needed this evaluation as a final step for probation. She was not in trouble in her job and in fact, highly regarded in her profession. Given the client was at the end of her requirements, the evaluator was somewhat concerned with the results and what it meant. The instructions were given to answer the FVA/FVOD side for the last twelve months. Her RAP is zero. Her Prescription Drug Scale is zero. She has ‘no’ on all the rules so came up with a Low Probability of having a Substance Use Disorder. However, her DEF of 9 is highly elevated. Elevated DEF scores increase the possibility of the SASSI missing individuals with a substance use disorder. Elevated DEF may also reflect situational factors. Note that the SAM is within the norm so it is probably more likely that her DEF is situational given the context. She also has an OAT score of ‘O’ and a SAT score of ‘2’. Both are below the 15th percentile. A low OAT indicates someone has difficulty acknowledging personal limitations or shortcomings. A low SAT indicates someone who might have a ‘chip’ on her shoulder, a hypersensitivity to others or feelings of rejection.

So even though this client is nearing the completion of her probation requirements, we still get a picture of someone who is highly guarded (DEF), has a hard time acknowledging shortcomings (OAT) and may continue to exhibit resentment (SAT) for the situation she is in. Perhaps this is due to her profession, or perhaps it is her personality. What the results give the evaluator is clinical direction on how to approach the client to help reduce her defensiveness and give her permission to open up. Affirming how demanding her job is and how on top of things she must be could be a pathway to discussing her feelings of shame related to the DWI and how it might be affecting her self-esteem. Could she be minimizing her use of alcohol and drugs? Perhaps, but as we strongly express, the SASSI is only one part of a clinician’s assessment. Hopefully, with the input of all the information you have, the clinician can evaluate the results which fit the context for this client.
A Review of a SASSI-4
The SASSI-4 I am reviewing is interesting for what it is not.
The client was instructed to complete the FVA/FVOD for the last 12 months.
The client is a 34 year old male with a history of drug and alcohol use. He reports that two and a half years ago he successfully completed treatment. He stopped doing drugs but continues to consume alcohol. He was being evaluated by the order of the court for an “altercation with his ex-spouse”. He does meet multiple rules and comes up with a high probability of a substance use disorder. Remember the number of Rules met does not mean a more significant disorder. The diagnosis is based on the DSM-5 with the designation of mild, moderate or severe based on the number of symptoms met.
As seen on the profile sheet, he has a number of elevated scales including the FVA, SYM, OAT, SAT and COR. What is interesting, is that his DEF is not elevated and is below average staying within the norm. For domestic violence cases, this is fairly unusual. Often we see an elevated DEF above the 85th percentile. The FVA and SYM scores indicate an openness and acknowledgment of his use as well as symptoms and consequences. The elevated SYM also indicates he is either hanging out with or from a family of heavy users. In this case, he disclosed his family has a history of alcohol abuse.
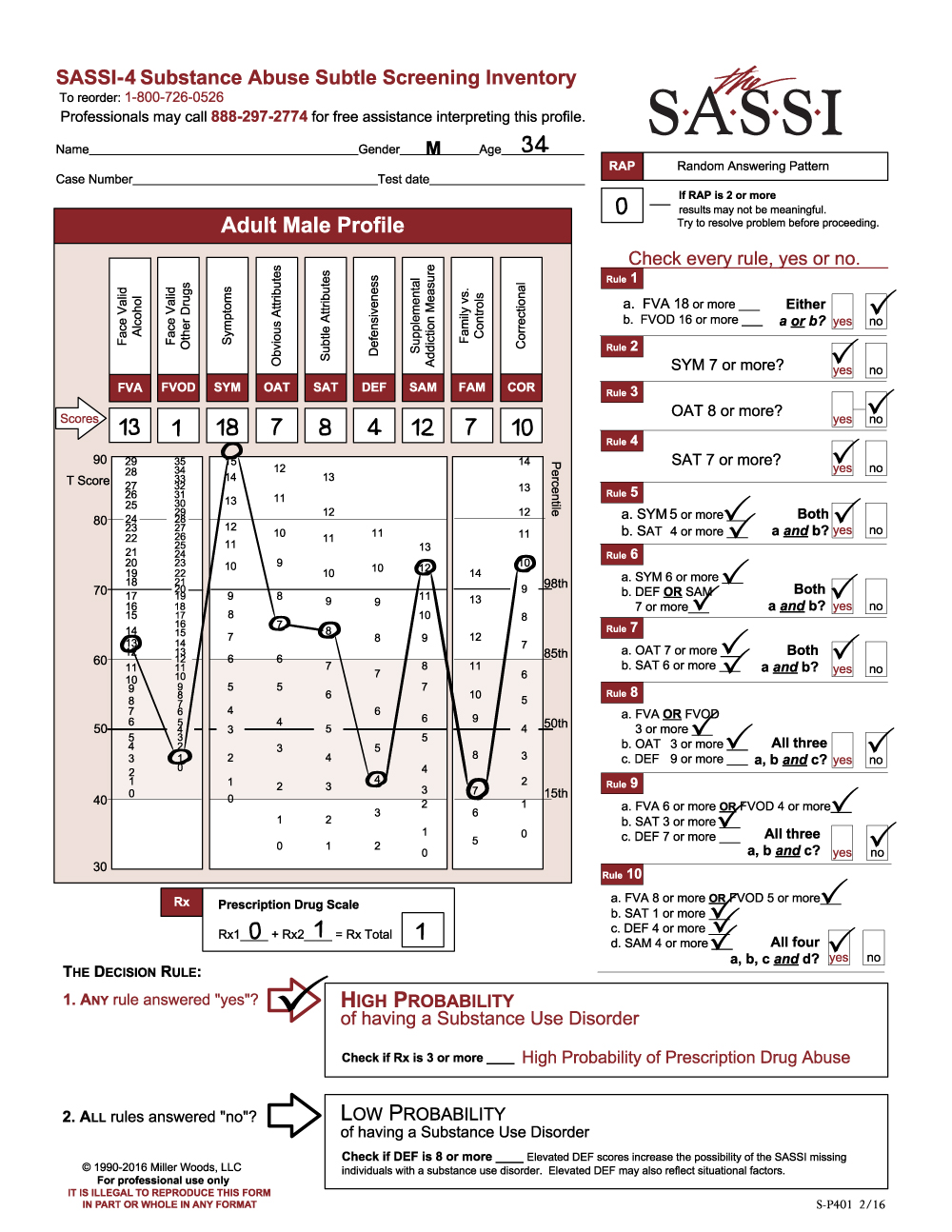
The elevated OAT score indicates that he can probably identify with other substance users and those behaviors we often see with substance abusers i.e. impatience, resentment, self-pity and impulsiveness. On the other hand, his elevated SAT indicates a lack of awareness or insight or simple denial of the impact alcohol is having on him. He readily acknowledges his past drug issues but has put alcohol in a separate category. His final elevated scale is COR. Regardless of any past or present legal issues, we encourage evaluating for those behaviors that impact the ability to make good choices. These behaviors can range from poor social skills, low frustration tolerance, risk-taking behaviors to impulse control or anger management issues.
Utilizing the results: The evaluation started out as a domestic violence case but transitioned to also include substance use. The fact that the client was open about his alcohol use, not defensive and has a successful treatment history suggests he may be willing to take a look at his alcohol use and its impact on his behavior. His elevated OAT score does indicate treatment readiness and he is not going to feel out of place in a group setting. The emphasis will be to help him connect the dots between his alcohol use and any impulsive behaviors. This does not take the place of any recommended intervention for anger management issues he may have. The administrator has a good opportunity to facilitate the client to continue the work needed on his recovery and deal with all his issues.
We hope this is helpful for you in your work with your clients. As usual, the free clinical helpline is open for your questions M-F, 11-5, (EST). Don’t hesitate to call us whether you are new to the SASSI or an old hand.