The SASSI Institute’s Clinical Help Line is a free resource designed to support clinicians and professionals using the Substance Abuse Subtle Screening Inventory (SASSI). It provides assistance with clinical interpretation of scores on each of the SASSI scales; helps individuals understand typical trends seen in SASSI profiles and how to use that information in educating clients, making referrals for clients, or developing treatment plans; provides assistance in manual scoring issues; and addresses any other specific SASSI-related questions.
Typical Clinical Help Line services include:
· Clarifying how to interpret complex or ambiguous results.
· Answering questions about the SASSI tools’ methodology or scoring.
· Providing recommendations for follow-up based on screening results.
· Offering advice on integrating SASSI assessments into broader treatment planning.
This service helps clinicians maximize the effectiveness of the SASSI tools in identifying and addressing substance use issues in diverse client populations. The Clinical Help Line is staffed by experienced, licensed/certified professionals with many years of experience and expertise in the SASSI instruments, substance use disorders and screening and assessment. They are available to answer your questions Monday thru Friday from 1:00pm to 5:00pm EST. This is a totally free service so give our friendly clinicians a call and allow us to help you make your experience with the SASSI even better for you and your clients!
In a world increasingly dominated by virtual interactions, the value of face-to-face, hands-on training cannot be overstated. Onsite SASSI training offers unparalleled opportunities to immerse yourself in a dynamic learning environment that sparks creativity, fosters meaningful connections, and enhances your skillset.
Why Choose Onsite Training?
Personal Interaction: Engage directly with experienced trainers and fellow participants, creating a rich learning experience.
Hands-On Experience: Participate in practical exercises and real-time problem-solving that solidify your understanding and application of key concepts.
Immediate Feedback: Receive instant, personalized feedback from trainers, allowing you to refine your skills on the spot.
Networking Opportunities: Build lasting professional relationships with peers who share your commitment to excellence and growth.
Take the Next Step:
Ready to make a positive impact on your staff? Email me, Wallace Jones (an independent Certified SASSI Training contractor), via email wj1856@yahoo.com, by phone: 561.570.2118, or via WhatsApp: 849.707.8886, for your next onsite SASSI training sessions. Your staff will thank you!
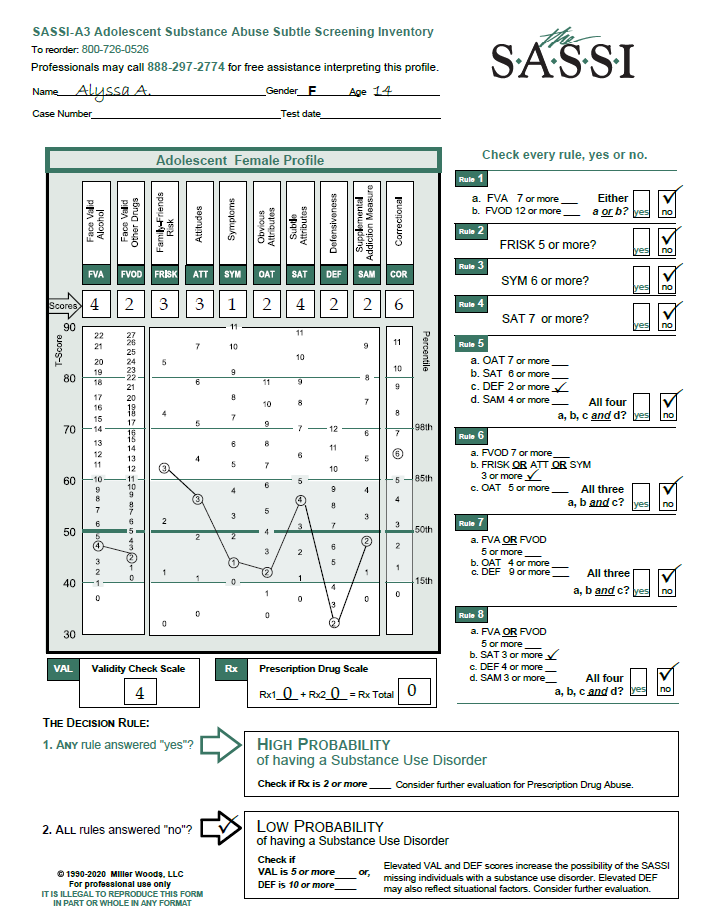
Alyssa (revised) is a 14-year-old female adolescent sent for evaluation by her teachers after noticing significant changes in her emotions and behavior. Her demeanor has gradually changed from a smiling, mostly compliant teen to that of a more rebellious and sullen one. She’s been caught skipping school a few times and was found to be in the company of some older adolescents who are consistently in trouble and suspected of using alcohol and drugs. The SASSI-A3 classified Alyssa with a LOW PROBABILITY of having a substance use disorder (SUD). Neither the VAL or DEF scale scores met the criteria for the possibility of a false negative. While the scale scores do not meet the criteria for classifying her as high probability of having an SUD, there are some other scale scores which could indicate some other clinical issues that may need to be addressed.
In going beyond the decision rules and looking at the individual raw scale scores, it is possible to develop a more general hypothesis regarding her level of adjustment and functioning. The fact that she scored above a zero (0) on the FVA, FVOD and SYM scales tells us that, while her scores are not high enough to indicate the probability of an SUD and are in fact very close to the mean, at 14 years old she has used both alcohol and drugs and experienced some negative consequences and/or problems as a result of that use. Based on her elevated FRISK score of 3, her slightly elevated ATT score of 3 and her elevated COR score of 6 (along with the observations made by her teachers), we can further hypothesize that Alyssa is likely to be surrounded by a close social system who are abusing substances and, as a result of this, her attitudes toward substance use lean more toward endorsing and promoting such use as a good thing. Assuming that this social system likely consists of her peers, namely the older teens mentioned earlier, this may explain her elevated COR scale score. In other words, she may have similar thinking patterns, beliefs, values and attitudes as those who are more likely to engage in rule-breaking, unlawful behaviors and/or disdain for authority. Her OAT score seems to indicate that Alyssa does not at all identify with any of the typical attributes that we would normally associate with an active substance abuser and that she firmly believes that she does not have a substance use problem. One of the most concerning scale scores on this profile is the DEF score of 2. SASSI research tells us that very low DEF scores such as this, often indicate a young woman who is experiencing a great deal of emotional pain and many of the typical symptoms associated with a syndrome of clinical depression. She may tend to engage in negative self-statements, identifying herself as a loser or misfit. She may be experiencing a sense of hopelessness, inability to enjoy positive experiences, lethargy, general bad feelings, impaired functioning in vital areas such as sleeping and eating, and sometimes even suicidal ideation.
While a low DEF score is not a clinical diagnosis in itself, this profile raises some questions that a counselor may wish to pursue in an interview or further ongoing assessment. For example, what is causing the significant change in emotion and behavior that was noticed by the teachers? Is it simply the normal emotional volatility of a growing and changing adolescent? Is there something happening in this teenager’s family which has caused this sudden shift in emotion and acting out? In any case, hopelessness, suicidal ideation, depressive symptoms or other psychiatric problems are important concerns to be investigated. It would also be valuable to explore the extent and context of her drinking and drug use to determine if it is just normal adolescent experimentation, a reaction to peer pressure, or an attempt to deal with emotions too overwhelming to control on her own. While the SASSI does not indicate a high probability of having an SUD currently, without some sort of intervention regarding these sudden changes in emotions and behaviors, a future SUD problem is not out of the question. It is difficult to suggest appropriate interventions without further information. However, appears that she could benefit from seeing a safe, trustworthy and empathetic counselor who could further explore the issues and immediately address her emotional pain and help her develop coping skills other than alcohol and/or drugs. Using the raw scale score interpretations described previously, in an open two-way conversation the therapist and Alyssa could use these scores to begin to collaboratively develop a plan of action that could help her confront and overcome the difficulties she is facing.
We hope you find this useful information regarding clinical issues. As always, the Clinical Helpline at 888-297-2774 is open to serve you Monday through Friday, 1 pm to 5 pm (EST).
We invite you to join us for a free one-hour SASSI Clinical Q&A webinar hosted by our Clinical Director, David Helton, LMSW, LCDC. The Q&A is for those new to using the SASSI, those considering using the SASSI, or seasoned veterans at screening with the SASSI. The Q&A is scheduled from 11 am – Noon ET on: April 29th. You can save your spot by clicking here. We welcome you to share profiles to discuss with the group by sending them (de-identified) via email any time prior to the session to scarlett@sassi.com. These profiles will help others learn about SASSI and offer insight into the various profile configurations. Note: Q&A sessions do not provide CEUs and are not a substitute for SASSI Training.
Additionally, we will be hosting a Live online SASSI Training webinar on the Administration & Scoring of the web-based format of the SASSI (SASSI Online) as well as Clinical Interpretation in March. These sessions are $60 USD each and provide 3.5 CEUs. You can learn more and register by clicking here.
As we usher in another year, we at The SASSI Institute want to take a moment to reflect on the progress we’ve made together and share our excitement for the opportunities ahead. The start of a new year is not only a time for celebration but also a time to recommit ourselves to our mission of providing valid and reliable tools to support professionals in the substance use addiction field.
Whether you’re a seasoned professional or new to the field, we invite you to join us in making 2025 a year of impact and innovation. Stay connected by following us on our social media channels, attending our training workshops, participating in our free online clinical Q&A sessions, and sharing your insights with us.
Together, we can continue to build a future where every individual struggling with substance use receives the care and support they deserve. Let’s make this year one to remember—for all the right reasons.
We welcome you to join us for a free one-hour online SASSI Clinical Q&A session hosted by our Clinical Director, David Helton, LMSW, LCDC. Whether you’re new to the SASSI, considering using the SASSI, or a seasoned veteran at screening with the SASSI, everyone is welcome. The Q&A is scheduled from 11 am – Noon ET on: January14th. You can save your spot by clicking here. We welcome you to share profiles to discuss with the group by sending them (de-identified) via email any time prior to the session to scarlett@sassi.com. These profiles will help others learn about SASSI and offer insight into the various profile configurations. Note: Q&A sessions do not provide CEUs and are not a substitute for SASSI Training.
Additionally, we will be hosting a Live SASSI Training webinar on the Administration & Scoring of the paper & pencil format of the SASSI as well as Clinical Interpretation in December. The sessions are $60 USD each and provide 3.5 CEUs. You can learn more and register by clicking here.
We want clinicians to find the SASSI to be helpful in their work in a way that enables them to affect the lives of their clients in a positive manner.
When a client is unable to acknowledge (sincerely deluded) or unwilling to accept they may have a problem, a clinician’s skillful and caring feedback on SASSI results may help break through those barriers and enable the client to take the courageous step toward recovery.
If you would like to learn more about clinically interpreting SASSI profiles, we encourage you to join us for one of Clinical Interpretation trainings. For more information on live, on-demand, and in-person workshops, please visit https://sassi.com/sassi-training/
Free assistance interpreting SASSI results is available M-F 1-5 pm ET at 800.726-0526 Option 2.
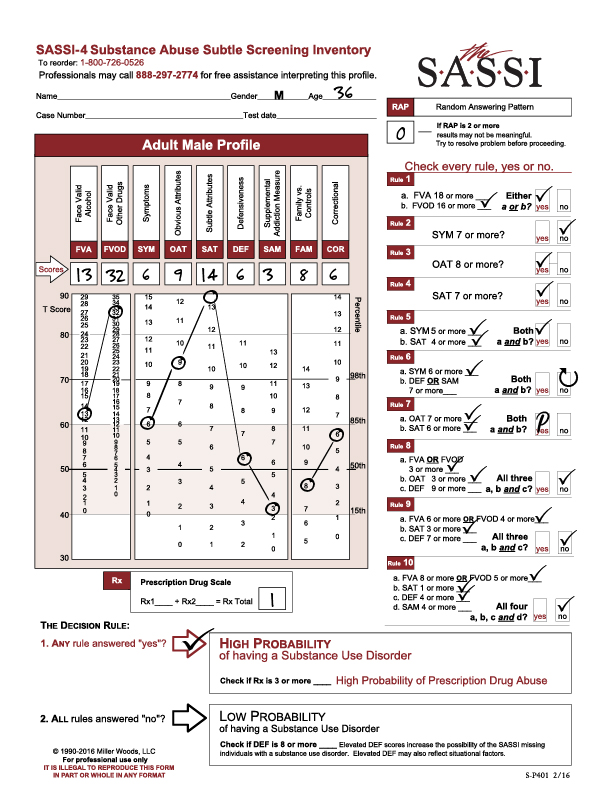
The following profile result is of a 35-year-old male referred for screening and possible assessment after a drug-related arrest. He completed the FVA/FVOD side of the questionnaire based on his entire life timeframe. His RAP score was 0, indicating no random responding and that the result should be valid. His Prescription Drug Scale score (Rx) was 1, so he did not meet the cutoff for High Probability of Prescription Drug Abuse.
Looking at this profile, we see that he was classified as high probability of a substance use disorder based on the following Decision Rules:
Decision Rule 1 with a FVOD score of 32.
Decision Rule 3 with an OAT score of 9.
Decision Rule 4 with a SAT score of 14.
Decision Rule 5 with a SYM score of 6 (5 or more) and a SAT score of 14 (4 or more).
Decision Rule 7 with an OAT score of 9 (7 or more) and a SAT score of 14 (6 or more).
Looking at the graph on the SASSI Adult Male Profile sheet, we see an extremely high elevation on the FVOD scale score which is significantly above the 98th percentile. Individuals who score this high on the FVOD are able to acknowledge currently having or having had numerous negative consequences and problems as a result of their use of drugs. This can include loss of control of the drug use as well as using a coping mechanism. It is important to note that, since he was asked to use the “entire life” timeframe for the FVA and FVOD scales, his admission of having these consequences and problems with drugs may be related to some time in his past and not necessarily currently. For example, the client’s score on the SYM scale (which is similar to the FVA/FVOD in what it is measuring), is not nearly as elevated as his score on the FVOD even though the questions are not that dissimilar from the FVOD questions.
This suggests that he is not showing as much acknowledgement on the SYM scale of the symptoms of substance misuse that he admitted to on the FVOD scale. This could be related to the fact that the SYM scale (like all scales on the True/False side of the questionnaire) has no specific timeframe associated with it and therefore the client may have the belief that, while he has had significant problems with drugs in the past, he may not believe his current drug use is as much of a problem currently. It is highly recommended that clinicians do a content analysis of the client’s answers to the FVOD and SYM scale questions as this will provide more insight into the client’s acknowledged problems with drugs.
This client’s elevated OAT scale score, like the elevated FVOD scale score, suggests a capacity to acknowledge and identify with many of the typical negative attributes (general personality and behavioral characteristics) and personal limitations that are often common among those with substance use disorders – e.g. impatience, resentment, self-pity, impulsiveness). While the client can often see these “character defects”, they may not always feel motivated to change them or feel capable of changing. Given that the OAT score in this case is above the 98th percentile, it is highly probable that this individual may be able to closely identify with individuals in recovery from substance use disorder, such as those found at recovery support groups, and therefore may be more willing to trust these recovering individuals and follow their recovery advice.
The client’s highly elevated SAT score (the highest score on this profile), which is higher on the graph than the OAT score, suggests that despite the client’s capacity to acknowledge the more obvious problems and negative consequences associated with his use of drugs, there are subtle aspects of his behavior, personality, and addiction that are extremely hard for him to acknowledge. In other words, he may not be able recognize the pervasiveness of his addiction, how it negatively affects and rules every aspect of his life with deeply held negative thinking patterns, beliefs and negative coping patterns driving his addictive behaviors.
Clients with a pattern of scores like this client who tend to be able to acknowledge heavy usage, negative consequences and problem behaviors, may still be convinced, sincerely deluded into thinking that they are not truly addicted. They will often present as more “superficial” saying things like “well, I go to work every day and do my job so I couldn’t be addicted”. Clients with elevated SAT scores (especially higher on the graph than their OAT score) tend to be more initially resistant to the need for treatment and are more likely to relapse. These clients tend to be detached from their feelings and have relatively little insight into the basis and causes of their problems (namely substance addiction). These clients typically need a more intensive level of treatment where they can receive constant support for their recovery efforts and can get the kind of group processing therapy needed to help them connect with their feelings and learn how to cope with them without drugs.
In providing treatment to this type of client it is important to recognize that underneath the many excuses (other than substance addiction) for their problems, there is an individual with a substance use disorder who is likely in pain and scared. Individuals with high SAT scores may not be in touch with the pain and fear, largely because they immediately numb any negative feelings with substances as soon as they appear, but the pain and fear. In this case, intensive treatment and group work has to be accompanied by sensitive and skillful clinical intervention that lets the individual know that somebody is aware of their fear deep within and that it will be a relief to let it out to begin healing.
We hope you find this useful information regarding clinical issues. As always, the Clinical Helpline at 888-297-2774 is open to serve you Monday through Friday, 9 am to 5 pm (EST).
Participants in our Clinical Interpretation (Session 2) of SASSI Training learn about screening and assessment information; giving client feedback; and practice interpretation using SASSI profiles. Upon completion of the session, participants should feel comfortable making clinical interpretations from both the adult SASSI-4 & adolescent SASSI-A3 scales and using the SASSI to engage the client in the treatment process.
Feedback to clients on SASSI profiles is useful in increasing awareness, eliciting further information, and establishing rapport. Presenting the results of the decision rules and discussing scale scores can help people come to grips with the significance of their substance usage and identify treatment goals.
The following is a link to a handout provided in the Clinical Interpretation Session that you are welcome to download for reference when interpreting profile: SASSI SCALES: CLINICAL FEEDBACK.
We encourage you to attend the Clinical Interpretation Session 2 of SASSI training if you have not already and to utilize our free Clinical phone line for consultation and help interpreting profiles at 800.726.0526 Option 2.
Substance use disorders cause problems for countless individuals and society as a whole. Alcohol and drug abuse often underlie difficulties presented as emotional, medical, family, school, or legal problems. These problems are not likely to be resolved until the underlying substance use problem is dealt with. Yet many affected individuals are unable or unwilling to acknowledge their misuse of psychoactive substances, and many human service providers lack the resources to conduct comprehensive diagnostic assessments for substance use disorders on every client in their practices.
Dr. Glenn A. Miller developed the SASSI in response to the need for a screening measure that could identify individuals with a high probability of having a substance use disorder, even if those individuals do not acknowledge substance misuse or symptoms associated with it.
The SASSI is brief, easy to administer, and objectively scored. A client can answer the questionnaire in less than fifteen minutes. The SASSI can be scored and interpreted in a minute or two.
Thus, clients with a high probability of having a substance use disorder can be identified and helped by employee assistance programs, vocational counselors, psychotherapists, medical personnel, criminal justice programs, and other human service providers.
The SASSI is used by human service practitioners throughout the United States and Canada, as well as other countries and is used to help over a million people every year. For information on the accuracy of our screening tools please visit https://sassi.com/reliability-validity/.
Extracted from: Lazowski, L. E., Kimmell, K.S., & Baker, S.L. (2016). The Adult Substance Abuse Subtle Screening Inventory-4 (SASSI-4) User Guide & Manual. Springville, IN: The SASSI Institute.