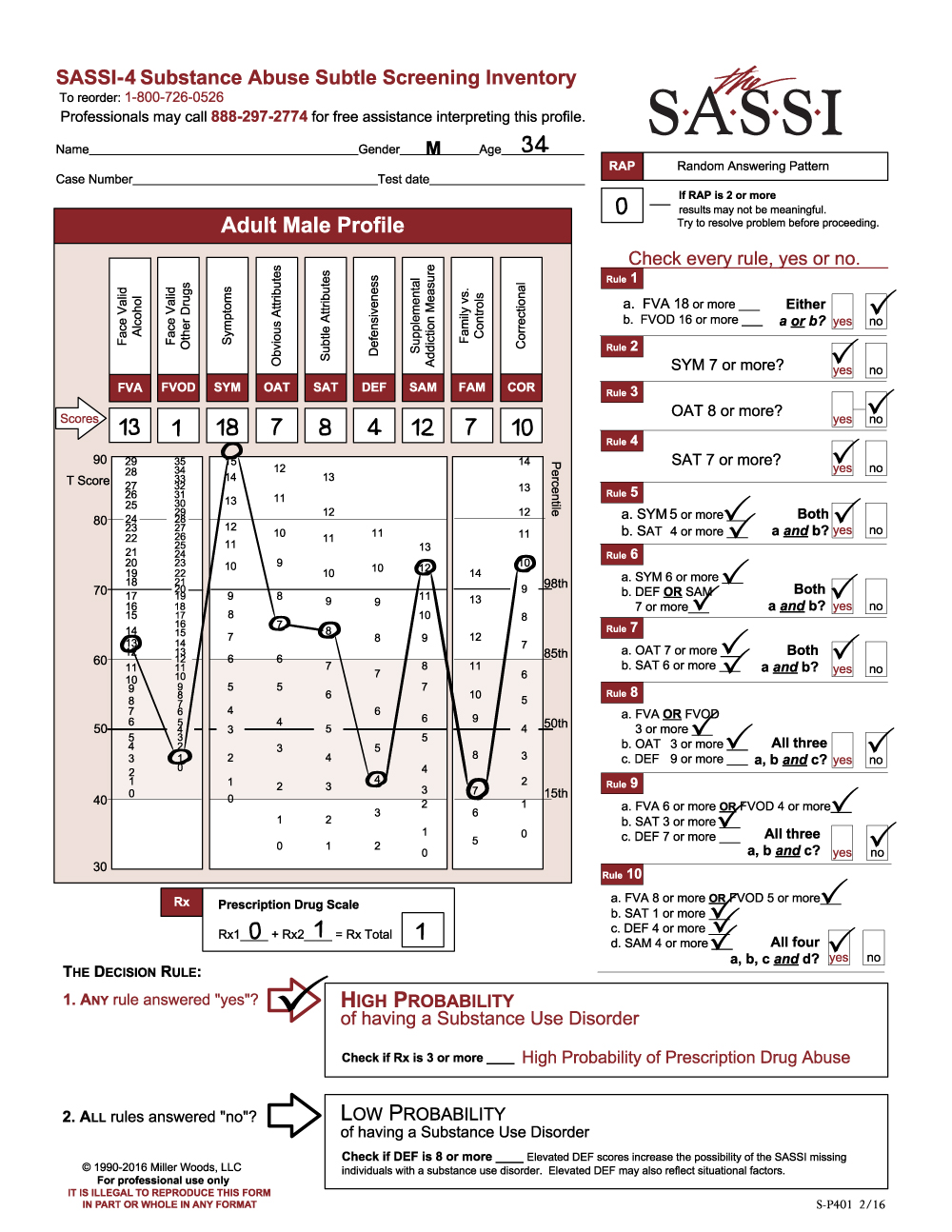
The following profile is for a 38-year-old male, “Blair,” who has been mandated to counseling following an instance of spousal abuse. First, note that the scale scores do not meet the criteria for classifying Blair as High Probability of having a substance use disorder (SUD). However, the Face-Valid Alcohol (FVA-12) and Face-Valid Other Drugs (FVOD-13) scores are moderately elevated above the mean (50th percentile) since they are more than one standard deviation from the mean and above the 85th percentile. It is important to recognize that FVA and FVOD are not just measures of frequency and quantity of consumption. Rather, they are mostly measures indicating acknowledgement of significant negative consequences as a result of substance misuse, as well as possible loss of control and using as a coping mechanism. Thus, even moderately elevated scores that do not in and of themselves lead to classifying the person as high probability of having a SUD are often indicative of some level of substance misuse. It is important to investigate this further. We not only want to establish whether substance misuse is a current or past pattern of use, but (in the context of this client’s reason for referral) further investigation is also needed to determine more about the relationship between physical abuse and substance misuse in this client’s life.
Note that the Obvious Attributes (OAT-1) score is low, i.e. it is below T40 where less than 15% of the normative sample typically scores. This type of OAT score suggests that Blair does not acknowledge the typical negative attributes or behaviors commonly associated with substance misusers such as impulse control problems, low frustration tolerance, impatience, a tendency to hold grudges, etc. An OAT score this low suggests it is not simply that he does not perceive himself as engaging in such behaviors, but that he actively (consciously or unconsciously) distances himself from any hint that he has such tendencies. In other words, he finds it difficult to acknowledge common weaknesses, personal limitations or human foibles and certainly does not see himself as being in any way similar to those who have substance problems. Often, people who come from homes that were dominated by abuse, substance misuse, or other problems are motivated to see themselves as not being like the primary abuser in their family of origin. His very elevated FAM score (FAM-14) and to some extent his somewhat elevated SYM (SYM-5) score suggest that he may have lived in an environment affected by substance misuse.
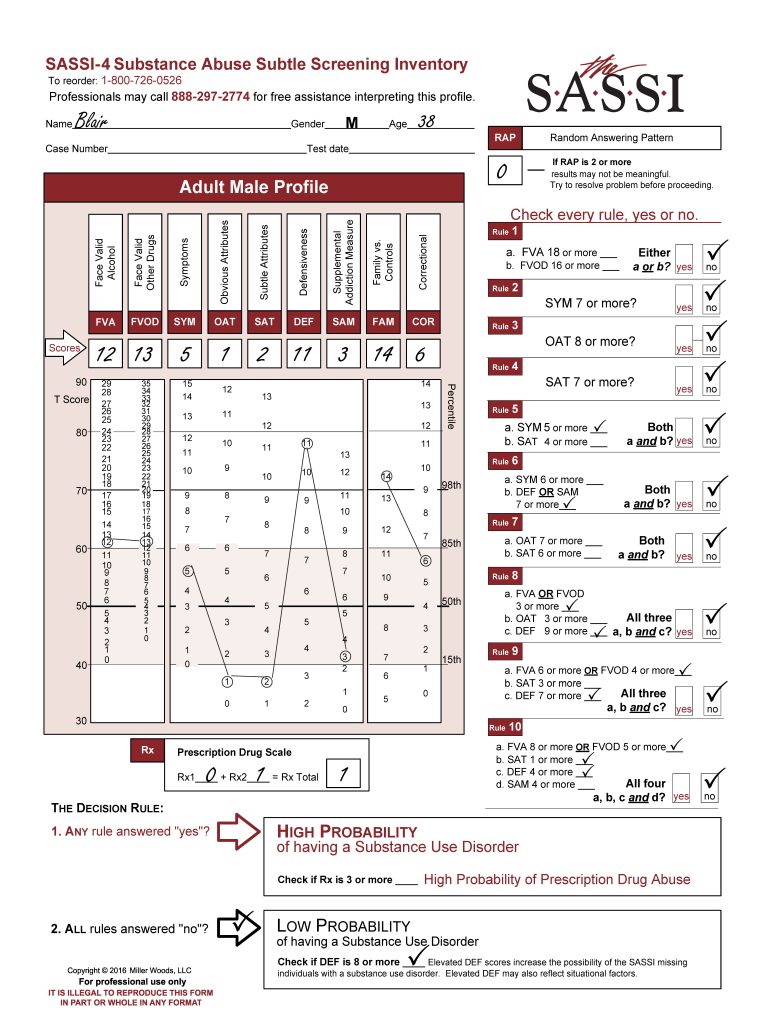
The Subtle Attributes (SAT-2) score is also significantly below average, and this can often indicate a person who may exhibit strong feelings of hypersensitivity to what others think of him stemming from his perception that others frequently reject him and unfairly judge and criticize him. This score suggests that Blair may be highly attuned to others’ opinions and may perceive slights or criticism, even when none are intended.
The Defensiveness score (DEF-11) is very significantly elevated. This often indicates someone who has their guard up and answers the questions by endorsing only things that may make them look more positive. This is not particularly abnormal in cases like Blair’s where there are situational factors putting him at risk of losing something important to him. Since Blair is being evaluated following an accusation that he beat his spouse, he is naturally on guard. The defensiveness could also reflect a more general tendency to avoid seeing and acknowledging any personal limitations or weaknesses and is somewhat confirmed by his very low OAT score as discussed earlier. Regardless of the cause, it is important to recognize that Blair probably approached the screening process in a defensive manner and because of this there is also a higher-than-normal possibility of a false negative and potentially a possibility that Blair minimized some of his symptoms of misuse on the more face valid scales such as the FVA, FVOD and SYM.
As mentioned earlier, Blair’s score on the Family vs. Controls (FAM-14) scale is significantly elevated. The FAM scale is composed of items that tend to identify individuals who may have been involved in a family of origin in which there was significant substance misuse. People who have high FAM scores often may obsessively focus on the needs and feelings of others. It is therefore interesting to contemplate how a high FAM score might fit as a characteristic of a perpetrator of domestic violence since spousal abusers are not generally thought of as “caretakers.” The crucial element may be the tendency of individuals who score high on the FAM scale to base their happiness and their sense of well-being on the behavior of others, leading to a need to control. Violence can be an extreme expression of a profound need to control.
Based on his SASSI scores, the Decision Rules result indicates a low probability of Blair being diagnosed as having a SUD. However, the significantly elevated DEF score cautions that there is an increased possibility of a false negative result (i.e. test-miss). His FVA and FVOD scores, while not high enough by themselves to provide a “high probability of a SUD” result, were clear indicators of acknowledged negative consequences from misuse of substances. Given the fact that many people with DEF scores as high as Blair’s often minimize some or a lot on the face valid scales to make themselves look better, there is still a possibility that Blair may suffer from a substance use disorder. Substance misuse is a common ingredient in domestic violence.
Domestic abusers often do not assume responsibility for their behavior, claiming that the victim “made me do it.” Blair’s SASSI profile corroborates and expands on this. The low SAT score suggests that Blair may have this victim mentality, and the low OAT score suggests that he is indisposed to see in himself the very tendencies that are likely to lead to spousal abuse such as low frustration tolerance, poor impulse control, anger management problems, a tendency to hold grudges, etc. The high-DEF score suggests a broader proclivity not to acknowledge personal limitations and to only endorse positives; and an extreme focus on others, as suggested by the high FAM score, could lead to an inability to deal effectively with interpersonal conflict. Ongoing comprehensive assessment should be directed toward determining more precisely the role of substance misuse in Blair’s spousal abuse. Treatment should also be directed toward helping Blair perceive and act in accord with appropriate personal boundaries. He is likely to need help in learning to accept and deal with interpersonal conflict and to assume greater responsibility for his behavior. As it stands, his extreme need to control others may lead to poor social judgment that allows him to construe violent acts as mature behavior and provides him with a rationale for excusing the inexcusable.
We hope you find this useful information regarding clinical issues. As always, the Clinical Helpline at 888-297-2774 is open to serve you Monday through Friday, 1 pm to 5 pm (EST).