We receive regular phone inquiries regarding which side of the Profile Sheet to use in scoring either the Adolescent or Adult SASSI when the client identifies as transgender or neither male nor female. This comes up whether one is using the paper and pencil or the online version.
To affirm one’s self-identity can be powerful and empowering so a discussion with a client who is either questioning their gender identification or sexual orientation or is very clear about either one can be a very supportive encounter. The message given is one of sensitivity, respect, and validation for their choices.
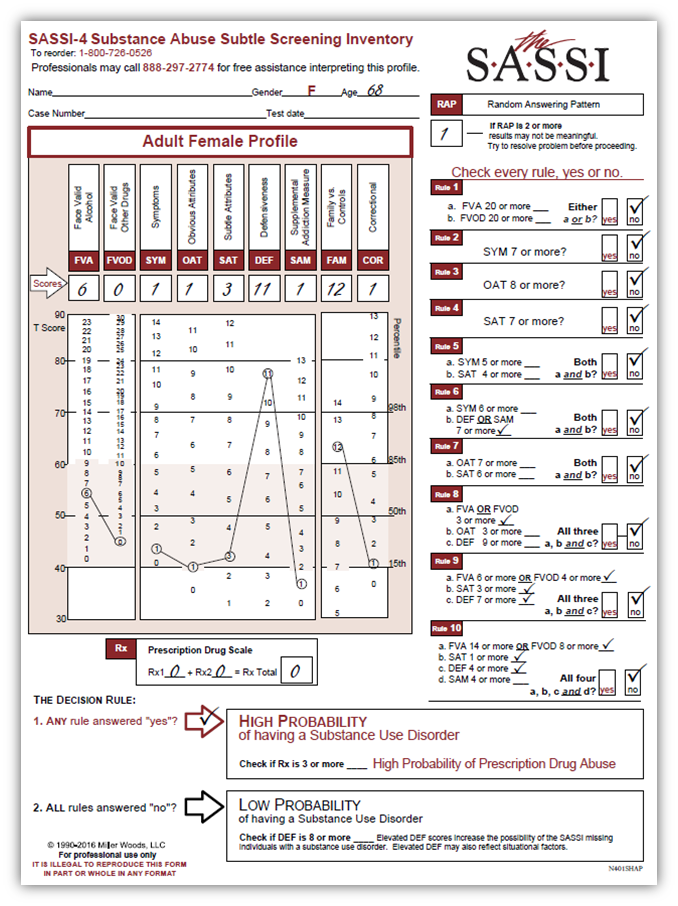
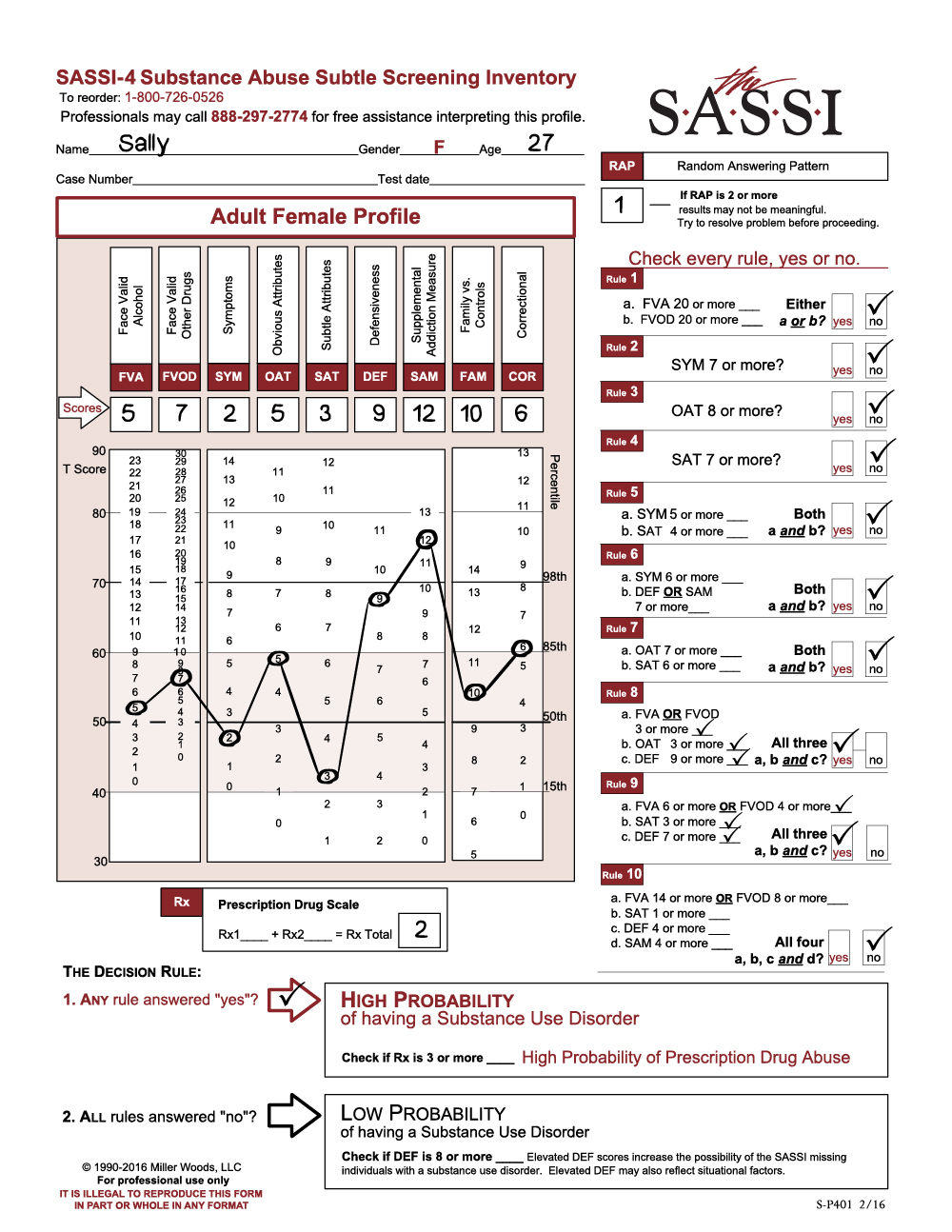
As a way of addressing this issue the adult SASSI-4, adolescent SASSI-A3, and Spanish SASSI ask for ‘gender’ in the demographics rather than ‘sex.’ This allows the client to indicate their self-identity. What side of the profile sheet used for scoring purposes should either (1) conform most closely to what the client indicates or (2) after discussion with the client, what they feel most comfortable with given the gender limitations of M/F on the SASSI. The research is based on binary identification and as such, we are limited in adding additional categories. Future research will undoubtedly be more inclusive. Regardless, the results are valid. The overall goal of the inventory is to give both the administrator and the client a compass to follow with useful information regarding the extent that substance use may or may not be a problem.
To be clear, score the side of the profile sheet that the transgender client self-identifies with. Not when or if they started hormones, or in a current state of transitioning, or they identified as a different gender when the legal offense happened.
A client may express a preference to not identify in any way and decline any gender identification. In that case, the administrator may want to score both sides of the SASSI to see if there is any difference in the result. More often than not, the result will be the same. The primary differences in M/F are in the FVA/FVOD scales which impact Rule 1 and Rule 10 in SASSI-4. There are no differences in the SASSI-A3.
The following is a list of LGBTQA terminology and definitions provided from the Prism Youth Community, part of Bloomington PRIDE here in Indiana:
These definitions were borrowed and adapted from several sources including the University of California- LA LGBT Campus Resource Center, the University of California Berkeley Gender Equity Resource Center, the University of Michigan Spectrum Center, and the University of Wisconsin Milwaukee LGBT Resource Center.
Definitions may vary with location, era, and culture. It is very important to respect people’s desired self-identifications. One should never assume another person’s identity based on that person’s appearance. It is always best to ask people how they identify, including what pronouns they prefer and to respect their wishes.
Ally – Typically any non-LGBT person who supports and stands up for the rights of LGBT people, though LGBT people can be allies, such as a lesbian who is an ally to a transgender person.
Androgyne – A person appearing and/or identifying as neither man nor woman, presenting a gender either mixed or neutral.
Asexual – A person who is not sexually attracted to any gender or does not have a sexual orientation. Asexuality is not the same as celibacy.
Bisexual or Bi – A person emotionally, physically, and/or sexually attracted to males/men and females/women. This attraction does not have to be equally split between genders and there may be a preference for one gender over others.
Cisgender – A person who feels comfortable with the gender identify and gender expression expectations assigned to them based on their physical sex.
Gender Expression – The way in which a person expresses their gender identity through clothing, behavior, posture, mannerisms, speech patterns, activities, and more.
Gender Identity – A person’s sense of being masculine, feminine, or other gendered.
Genderqueer A gender variant person whose gender identity is neither male nor female, is between or beyond genders, or is some combination of genders.
Homosexual or Gay – A person primarily emotionally, physically, and/or sexually attracted to members of the same sex.
Intersex – A person whose sexual anatomy or chromosomes do not fit with the traditional markers of “female” and “male”. For example: people born with both “female” and “male” anatomy (penis, testicles, vagina, uterus); people born with XXY.
Lesbian – A female-identified person attracted emotionally, physically, and /or sexually to other female-identified people.
LGBTIQA+ – Lesbian, gay, bisexual, transgender, intersex, queer, asexual or ally, and other identities.
Pansexual – A person who is sexually attracted to all or many gender expressions.
Partner – A significant other in an intimate relationship; a gender-neutral alternative to boyfriend/girlfriend, husband/wife, or other binary-based relationships terms.
Queer – 1. An umbrella term for people who are not heterosexual or cisgender. 2. A reclaimed word that was formerly used solely as a slur but that has been semantically overturned by some members of the LGBTIQA+ community, who use it as a term of defiant pride.
Sex – A medical term designating a certain combination of gonads, chromosomes, external gender organs, secondary sex characteristics and hormonal balances.
Sexual Orientation – The desire for intimate emotional and/or sexual relationships with people of the same gender/sex, another gender/sex, or multiple genders/sexes.
Sexuality – A person’s exploration of sexual acts, sexual orientation, sexual pleasure, and desire.
Trans – An abbreviation that is sometimes used to refer to a gender variant person. This use allows a person to state a gender variant identity without having to disclose hormonal or surgical status/intentions.
This term is sometimes used to refer to the gender variant community as a whole.
Transgender – An umbrella term for a person whose gender identity, expression or behavior is different from those typically associated with their assigned sex at birth.